Department of Orthopaedic Surgery, Hirosaki Memorial Hospital, Hirosaki, Japan.
Department of Orthopaedic Surgery, Hirosaki University Graduate School of Medicine, 5 Zaifu-cho, Hirosaki, Aomori, 036-8562, Japan.
Sci Rep. 2022 Mar 19;12(1):4756. doi: 10.1038/s41598-022-08604-3.
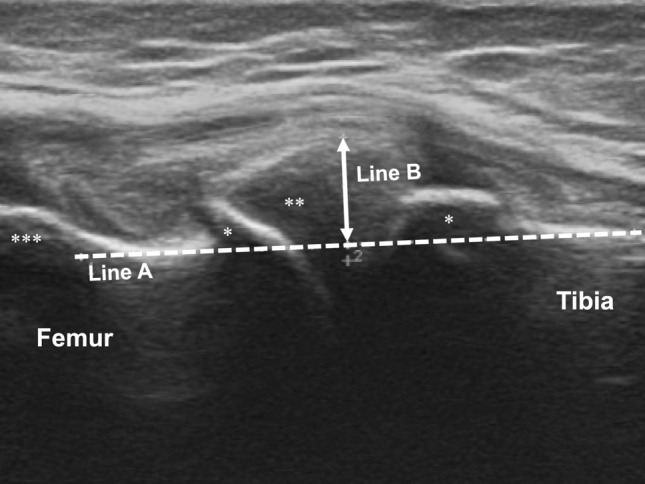
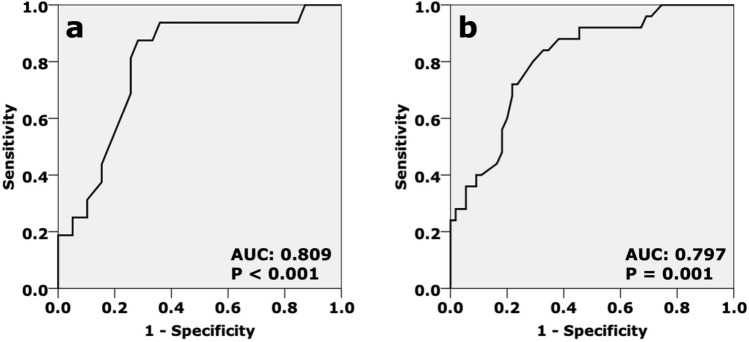
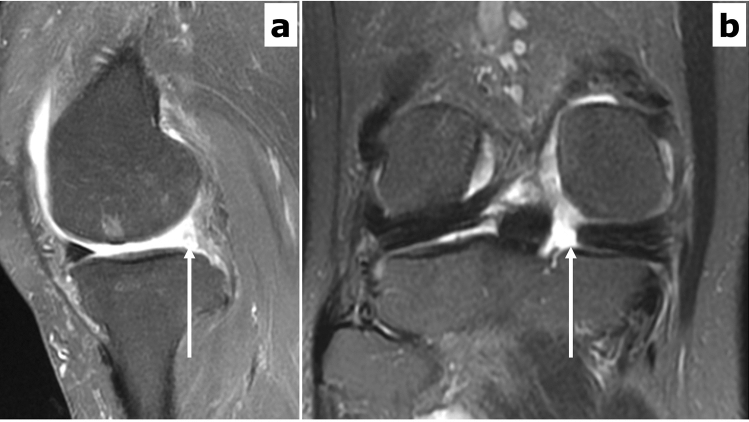
To elucidate the association between medial meniscus extrusion measured on ultrasonography (MME) and the prevalence of medial meniscus posterior root tear detected on magnetic resonance imaging (MMPRT). We recruited 127 patients (135 knees; 90 females; mean age: 64.4 ± 8.7 years old; mean BMI: 25.5 ± 3.4 kg/m) in this cross-sectional study. All participants had medial knee pain without a knee trauma or surgery history. Knee osteoarthritis (KOA) severity was evaluated using Kellgren-Lawrence grade (KLG) scores. Patients with KLG scores 0-1 and ≥ 2 were classified in non-radiographic (non-ROA) and radiographic KOA (ROA) groups, respectively. MME was measured with patients in the supine position. Based on fat-suppressed T2-weighted images, MMPRT was defined as the presence of "Ghost meniscus sign" and "Cleft/truncation sign", indicating an abnormal high signal intensity of a completely disrupted posterior root. MME was compared between MMPRT+ and MMPRT- patients using a non-paired t-test. Receiver operating characteristic (ROC) curves were used to determine the optimal cut-off MME to predict MMPRT+. The prevalence of MMPRT+ was 31.3% (25/80 knees) and 29.1% (16/55 knees) in the non-ROA and ROA groups. The MME of MMPRT+ patients were significantly greater than that of MMPRT- patients in both the non-ROA (5.9 ± 1.4 mm vs. 4.4 ± 1.0 mm, P < 0.001) and ROA (7.8 ± 1.3 mm vs. 6.3 ± 1.3 mm, P < 0.001) groups. ROC curves demonstrated that 5-mm and 7-mm MME were the optimal cut-off values in non-ROA (adjusted odds ratio: 6.280; area under the curve [AUC]: 0.809; P < 0.001) and ROA (adjusted odds ratio: 15.003; AUC: 0.797; P = 0.001) groups. In both early non-radiographic and established radiographic KOA stages, a greater MME was associated with a higher MMPRT prevalence.
为了阐明超声测量的内侧半月板挤压(MME)与磁共振成像(MMPRT)检测到的内侧半月板后根撕裂之间的关联。我们在这项横断面研究中招募了 127 名患者(135 膝;90 名女性;平均年龄:64.4±8.7 岁;平均 BMI:25.5±3.4 kg/m)。所有参与者均有内侧膝关节疼痛,无膝关节创伤或手术史。使用 Kellgren-Lawrence 分级(KLG)评分评估膝关节骨关节炎(KOA)严重程度。KLG 评分 0-1 和≥2 的患者分别归入非放射性(非 ROA)和放射性 KOA(ROA)组。MME 是在患者仰卧位时测量的。根据脂肪抑制 T2 加权图像,将 MMPRT 定义为“幽灵半月板征”和“裂隙/截断征”的存在,表明后根完全中断的异常高信号强度。使用非配对 t 检验比较 MMPRT+和 MMPRT-患者的 MME。使用受试者工作特征(ROC)曲线确定预测 MMPRT+的最佳 MME 截断值。MMPRT+的患病率为非 ROA 组 31.3%(25/80 膝)和 ROA 组 29.1%(16/55 膝)。MMPRT+患者的 MME 在非 ROA 组(5.9±1.4mm 比 4.4±1.0mm,P<0.001)和 ROA 组(7.8±1.3mm 比 6.3±1.3mm,P<0.001)中均显著大于 MMPRT-患者。ROC 曲线表明,5mm 和 7mm 的 MME 是非 ROA(调整后的优势比:6.280;曲线下面积[AUC]:0.809;P<0.001)和 ROA(调整后的优势比:15.003;AUC:0.797;P=0.001)组的最佳截断值。在早期非放射性和已建立的放射性 KOA 阶段,更大的 MME 与更高的 MMPRT 患病率相关。