Institute of Pathology, Friedrich-Alexander-University Erlangen-Nürnberg, University Hospital, Erlangen, Germany.
Head Neck Pathol. 2022 Mar;16(1):168-178. doi: 10.1007/s12105-022-01416-x. Epub 2022 Mar 21.
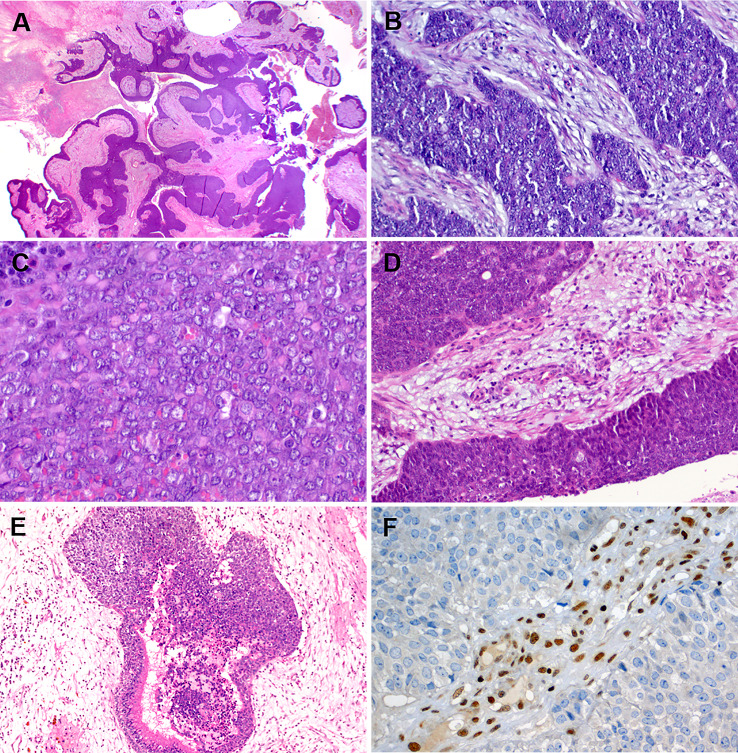
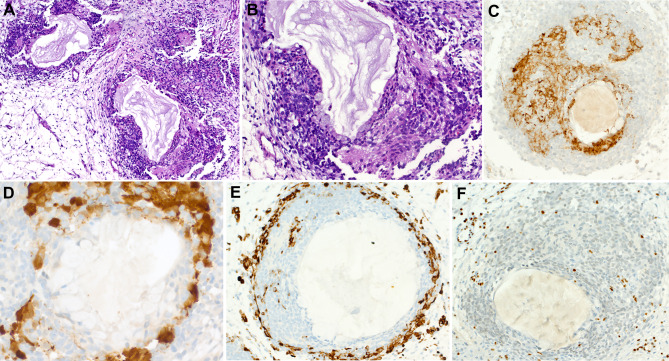
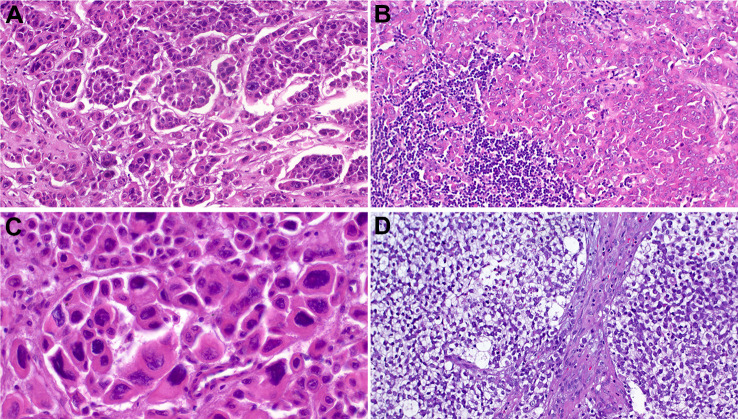
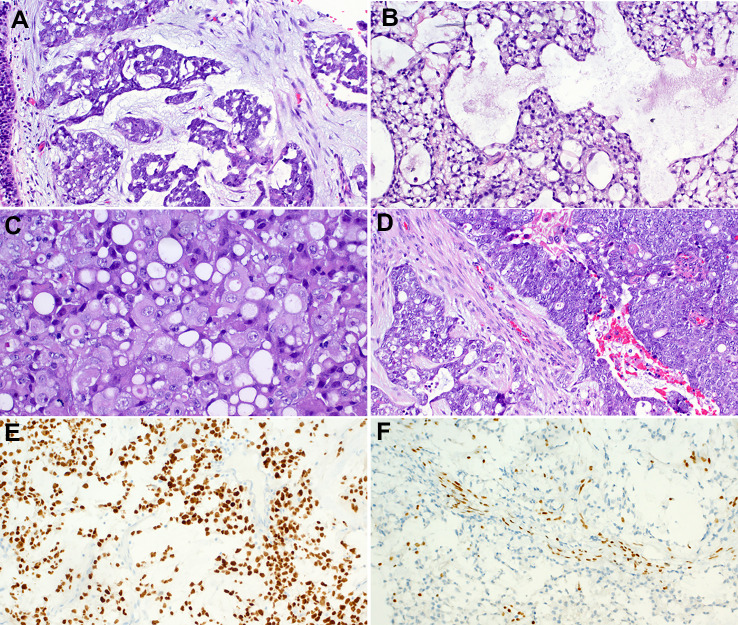
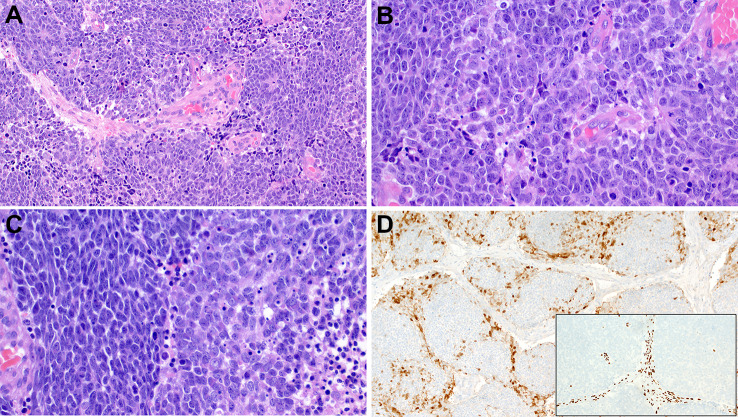
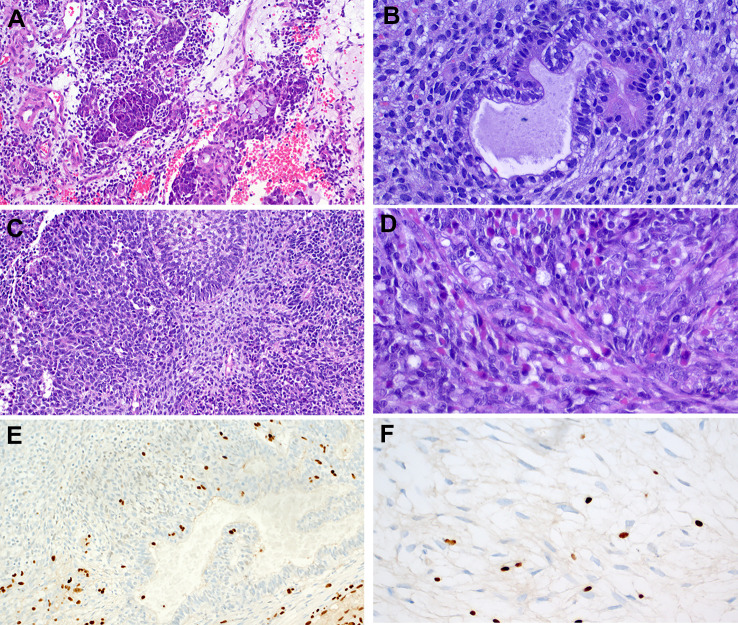
The pathology of poorly differentiated sinonasal malignancies has been the subject of extensive studies during the last decade, which resulted into significant developments in the definitions and histo-/pathogenetic classification of several entities included in the historical spectrum of "sinonasal undifferentiated carcinomas (SNUC)" and poorly differentiated unclassified carcinomas. In particular, genetic defects leading to inactivation of different protein subunits in the SWI/SNF chromatin remodeling complex have continuously emerged as the major (frequently the only) genetic player driving different types of sinonasal carcinomas. The latter display distinctive demographic, phenotypic and genotypic characteristics. To date, four different SWI/SNF-driven sinonasal tumor types have been recognized: SMARCB1(INI1)-deficient carcinoma (showing frequently non-descript basaloid, and less frequently eosinophilic, oncocytoid or rhabdoid undifferentiated morphology), SMARCB1-deficient adenocarcinomas (showing variable gland formation or yolk sac-like morphology), SMARCA4-deficient carcinoma (lacking any differentiation markers and variably overlapping with large cell neuroendocrine carcinoma and SNUC), and lastly, SMARCA4-deficient sinonasal teratocarcinosarcoma. These different tumor types display highly variable immunophenotypes with SMARCB1-deficient carcinomas showing variable squamous immunophenotype, while their SMARCA4-related counterparts lack such features altogether. While sharing same genetic defect, convincing evidence is still lacking that SMARCA4-deficient carcinoma and SMARCA4-deficient teratocracinosarcoma might belong to the spectrum of same entity. Available molecular studies revealed no additional drivers in these entities, confirming the central role of SWI/SNF deficiency as the sole driver genetic event in these aggressive malignancies. Notably, all studied cases lacked oncogenic IDH2 mutations characteristic of genuine SNUC. Identification and precise classification of these entities and separating them from SNUC, NUT carcinoma and other poorly differentiated neoplasms of epithelial melanocytic, hematolymphoid or mesenchymal origin is mandatory for appropriate prognostication and tailored therapies. Moreover, drugs targeting the SWI/SNF vulnerabilities are emerging in clinical trials.
过去十年中,低分化鼻窦恶性肿瘤的病理学已成为广泛研究的课题,这导致了历史上“未分化鼻窦癌(SNUC)”和低分化未分类癌范围内的几个实体的定义和组织/发病机制分类发生了重大变化。特别是,导致 SWI/SNF 染色质重塑复合物中不同蛋白亚基失活的遗传缺陷不断出现,成为驱动不同类型鼻窦癌的主要(通常是唯一)遗传因素。后者表现出独特的人口统计学、表型和基因型特征。迄今为止,已经认识到四种不同的 SWI/SNF 驱动的鼻窦肿瘤类型:INI1 缺失型癌(通常表现为非典型基底样形态,较少表现为嗜酸性、oncocytoid 或横纹肌样未分化形态)、INI1 缺失型腺癌(表现为可变的腺体形成或卵黄囊样形态)、SMARCA4 缺失型癌(缺乏任何分化标志物,与大细胞神经内分泌癌和 SNUC 部分重叠),最后是 SMARCA4 缺失型鼻窦胚胎性癌肉瘤。这些不同的肿瘤类型表现出高度可变的免疫表型,INI1 缺失型癌表现出可变的鳞状免疫表型,而其 SMARCA4 相关的对应物则完全缺乏这种特征。尽管存在相同的遗传缺陷,但仍然缺乏令人信服的证据表明 SMARCA4 缺失型癌和 SMARCA4 缺失型胚胎性癌肉瘤可能属于同一实体的范围。现有的分子研究表明这些实体中没有其他驱动因素,这证实了 SWI/SNF 缺陷作为这些侵袭性恶性肿瘤唯一驱动遗传事件的核心作用。值得注意的是,所有研究病例均缺乏真正的 SNUC 特征性的致瘤性 IDH2 突变。这些实体的鉴定和精确分类,以及将其与 SNUC、NUT 癌和其他上皮性、黑色素细胞性、造血淋巴样或间质性起源的低分化肿瘤区分开来,对于适当的预后和针对性治疗是必要的。此外,针对 SWI/SNF 脆弱性的药物正在临床试验中出现。