Karlsson Niklas, Berglund Torsten, Ekström Anna Mia, Hammarberg Anders, Tammi Tuukka
Department of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden; and Department of Public Health Analysis and Development, Public Health Agency of Sweden, Solna, Sweden.
Department of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden; and Department of Medicine Huddinge, Division of Infectious Diseases, Karolinska Institutet, Karolinska University Hospital Huddinge, Stockholm, Sweden.
Nordisk Alkohol Nark. 2021 Feb;38(1):66-88. doi: 10.1177/1455072520965013. Epub 2020 Dec 17.
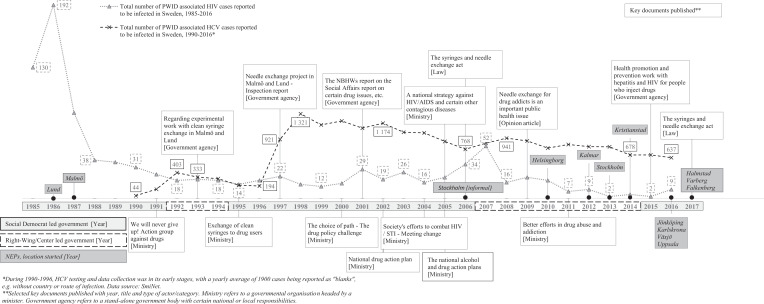
To end the hepatitis and AIDS epidemics in the world by 2030, countries are encouraged to scale-up harm reduction services and target people who inject drugs (PWID). Blood-borne viruses (BBV) among PWID spread via unsterile injection equipment sharing and to combat this, many countries have introduced needle and syringe exchange programmes (NEP), though not without controversy. Sweden's long, complicated harm reduction policy transition has been deviant compared to the Nordic countries. After launch in 1986, no NEP were started in Sweden for 23 years, the reasons for which are analysed in this study.
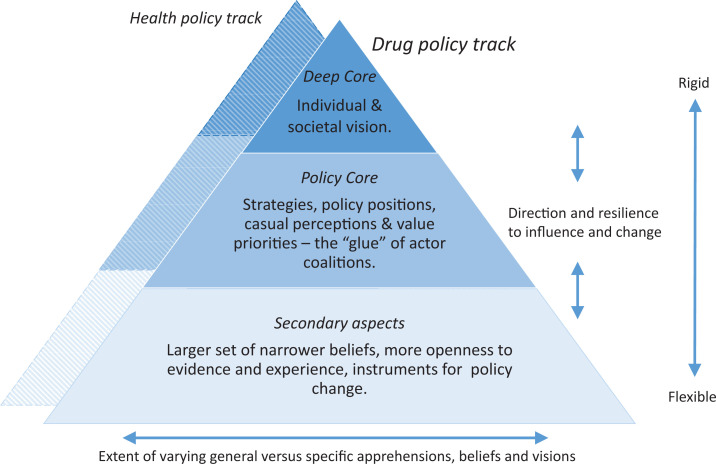
Policy documents, grey literature and research mainly published in 2000-2017 were collected and analysed using a hierarchical framework, to understand how continuous build-up of evidence, decisions and key events, over time influenced NEP development.
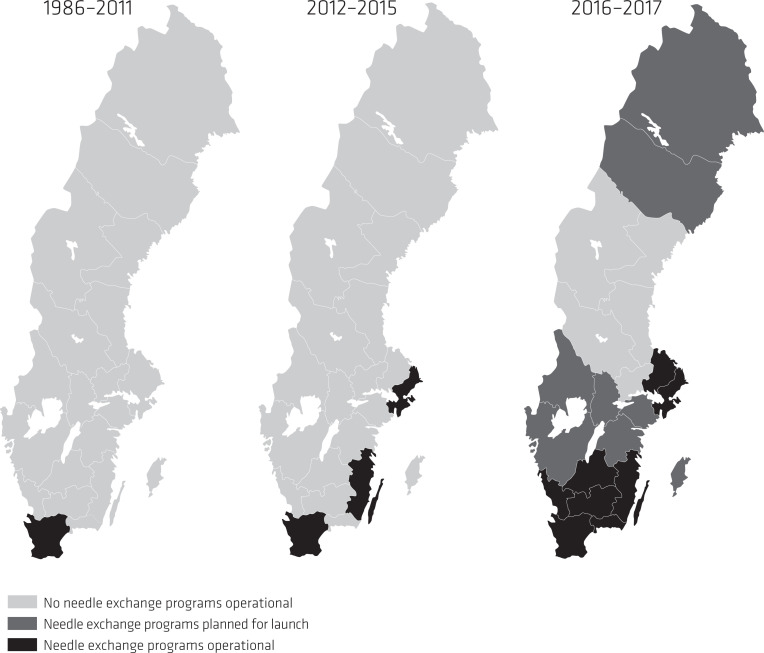
Sweden's first NEP opened in a repressive-control drug policy era with a drug-free society goal. Despite high prevalence of BBV among PWID with recurring outbreaks, growing research and key-actor support including a NEP law, no NEP were launched. Political disagreements, fluctuating actor-coalitions, questioning of research, and a municipality veto against NEP, played critical roles. With an individual-centred perspective being brought into the drug policy domain, the manifestation of a dual drug and health policy track, a revised NEP law in 2017 and removal of the veto, Sweden would see fast expansion of new NEP.
Lessons from the Swedish case could provide valuable insight for countries about to scale-up harm reduction services including how to circumvent costly time- and resource-intensive obstacles and processes involving ideological and individual moral dimensions.
为在2030年前终结全球的肝炎和艾滋病流行,鼓励各国扩大减少伤害服务,并以注射吸毒者为目标人群。注射吸毒者中的血源性病毒通过共用未经消毒的注射设备传播,为应对这一情况,许多国家推行了针头和注射器交换计划(NEP),不过并非没有争议。与北欧国家相比,瑞典漫长而复杂的减少伤害政策转型较为特殊。1986年该计划启动后,瑞典有23年未启动新的针头和注射器交换计划,本研究分析了其中的原因。
收集了主要发表于2000年至2017年的政策文件、灰色文献和研究资料,并使用分层框架进行分析,以了解随着时间推移,证据、决策和关键事件的持续积累如何影响针头和注射器交换计划的发展。
瑞典首个针头和注射器交换计划在以建立无毒品社会为目标的压制性控制毒品政策时代开启。尽管注射吸毒者中血源性病毒感染率很高且疫情反复爆发,研究不断增加,包括针头和注射器交换计划法在内的关键行为体也给予支持,但仍未启动新的针头和注射器交换计划。政治分歧、行为体联盟的波动、对研究的质疑以及一个市政府对针头和注射器交换计划的否决起到了关键作用。随着以个人为中心的视角进入毒品政策领域,出现了毒品和健康政策的双重轨道,2017年修订了针头和注射器交换计划法并取消了否决权,瑞典的新针头和注射器交换计划得以迅速扩展。
瑞典案例的经验教训可为即将扩大减少伤害服务的国家提供宝贵见解,包括如何规避涉及意识形态和个人道德层面的代价高昂、耗费时间和资源的障碍及过程。