Mielke Nicholas, Johnson Steven, Bahl Amit
Oakland University William Beaumont School of Medicine, Royal Oak, MI, USA.
Department of Emergency Medicine, Beaumont Hospital, 3601 13 Mile Rd, Royal Oak, MI 48073, USA.
Lancet Reg Health Am. 2022 Apr;8:100227. doi: 10.1016/j.lana.2022.100227. Epub 2022 Mar 17.
Real-world data on the effectiveness of boosters against COVID-19, especially as new variants continue to emerge, is limited. Our objective was to assess demographic, clinical, and outcome variables of patients requiring hospitalization for severe SARS-CoV-2 infection comparing fully vaccinated and boosted (FV&B), fully vaccinated (FV), and unvaccinated (UV) patients.
This multicenter observational cohort analysis compared demographic, clinical, and outcome variables in FV&B, FV, and UV adults hospitalized for COVID-19. Partially vaccinated (PV) and individuals still hospitalized beyond the designated follow-up date of February 1, 2022 were excluded. The primary endpoint was in-hospital mortality. Secondary endpoints included characteristics and outcomes in subpopulations of intensive care and geriatric (age >65) patients.
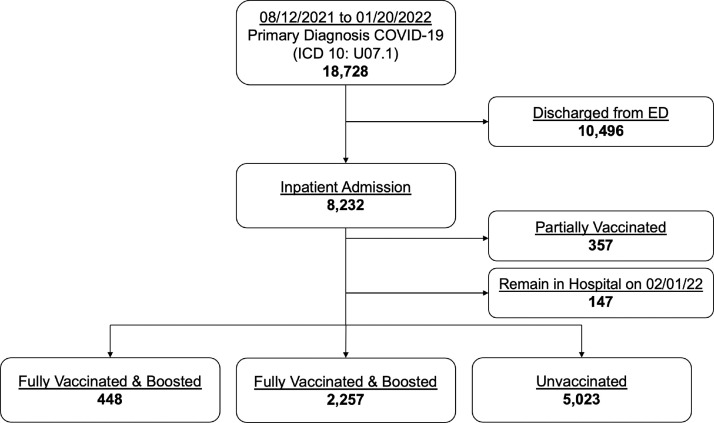
Between August 12th, 2021 and January 20th, 2022, 8232 patient encounters had a primary diagnosis of COVID-19 and required inpatient treatment. Of the 8232 encounters requiring hospitalization, 448 (5.8%) were FV&B, 2257 (29.2%) were FV, and 5023 (65.0%) were UV; 357 PV and 147 still hospitalized were excluded. The median age of FV&B cohort was 73 (IQR 62, 82) compared to 70 (IQR 59, 80) for FV and 59 (IQR 45, 71) for UV (0.001). Most patients were female in both the FB&V and UV groups with 51.1% and 51.8%, respectively, while the FV group had a majority of males (51.3%). The median Elixhauser weighted score was 12 (IQR 3, 22) for FV&B, 10 (IQR 2, 20) for FV, and 9 (IQR 0, 17) for UV groups ( < 0.001). In-hospital mortality was 7.1% in the FV&B, 10.3% in the FV group, and 12.8% in the UV group ( < 0.001). The FV&B group had lower in-hospital mortality than both FV and UV groups ( = 0.045 and = 0.001, respectively). The FV group had lower in-hospital mortality than the UV group ( = 0.004).
Fully vaccinated and boosted patients requiring hospital-level care for breakthrough COVID-19 have lower in-hospital mortality than fully vaccinated and unvaccinated patients despite being older and higher risk at baseline. Boosters offer added protection beyond full vaccination in preventing death. As COVID-19 continues to spread, larger expansive trials are needed to further identify risk factors for severe outcomes among the FV&B population.
This research received no specific grant from any funding agency in public, commercial, or not-for-profit sectors.
关于加强针预防新冠病毒病有效性的真实世界数据有限,尤其是在新变种不断出现的情况下。我们的目标是评估因严重SARS-CoV-2感染而需要住院治疗的患者的人口统计学、临床和结局变量,比较全程接种疫苗并接种加强针(FV&B)、全程接种疫苗(FV)和未接种疫苗(UV)的患者。
这项多中心观察性队列分析比较了因新冠病毒病住院的FV&B、FV和UV成年人的人口统计学、临床和结局变量。排除了部分接种疫苗(PV)的患者以及在2022年2月1日指定随访日期后仍住院的患者。主要终点是院内死亡率。次要终点包括重症监护亚组和老年(年龄>65岁)患者的特征和结局。
在2021年8月12日至2022年1月20日期间,8232例患者的主要诊断为新冠病毒病且需要住院治疗。在8232例需要住院治疗的患者中,448例(5.8%)为FV&B,2257例(29.2%)为FV,5023例(65.0%)为UV;排除了357例PV患者和147例仍住院的患者。FV&B队列的中位年龄为73岁(四分位间距62, 82),FV组为70岁(四分位间距59, 80),UV组为59岁(四分位间距45, 71)(P<0.001)。FV&B组和UV组的大多数患者为女性,分别占51.1%和51.8%,而FV组男性居多(51.3%)。FV&B组的Elixhauser加权评分中位数为12(四分位间距3, 22);FV组为10(四分位间距2, 20);UV组为9(四分位间距0, 17)(P<0.001)。FV&B组的院内死亡率为7.1%,FV组为10.3%,UV组为12.8%(P<0.001)。FV&B组的院内死亡率低于FV组和UV组(分别为P=0.045和P=0.001)。FV组的院内死亡率低于UV组(P=0.004)。
尽管全程接种疫苗并接种加强针的患者在基线时年龄更大、风险更高,但因突破性新冠病毒病需要住院治疗的此类患者的院内死亡率低于全程接种疫苗和未接种疫苗的患者。加强针在预防死亡方面提供了超过全程接种疫苗的额外保护。随着新冠病毒病继续传播,需要进行更大规模的扩展性试验,以进一步确定FV&B人群中严重结局的危险因素。
本研究未获得公共、商业或非营利部门任何资助机构的特定资助。