Gribsholt Sigrid Bjerge, Farkas Dóra Körmendiné, Thomsen Reimar Wernich, Richelsen Bjørn, Sørensen Henrik Toft
Department of Endocrinology and Internal Medicine, Aarhus University Hospital, Aarhus, Denmark.
Steno Diabetes Center, Aarhus University Hospital, Aarhus, Denmark.
Clin Epidemiol. 2022 Mar 14;14:309-325. doi: 10.2147/CLEP.S350459. eCollection 2022.
Data on long-term mortality among patients with hospital-diagnosed overweight/obesity are limited. Thus, we aim to examine 40-year mortality among patients with hospital-diagnosed overweight/obesity, including cause-specific deaths, secular time trends, and potential effect modification by age, comorbidity, and socioeconomic factors.
From national registries, we identified all Danes with a first hospital-based overweight/obesity diagnosis (N=331,185), 1979-2018, and constructed an age- and gender-matched general population comparison cohort (N=1,655,925). We computed mortality rates (MRs) per 1000 person-years and adjusted mortality rate ratios (aMRRs) with 95% confidence intervals (CIs), using Cox regression with adjustment for comorbidities and educational level. We performed stratified analyses on age, comorbidities, and socioeconomic factors.
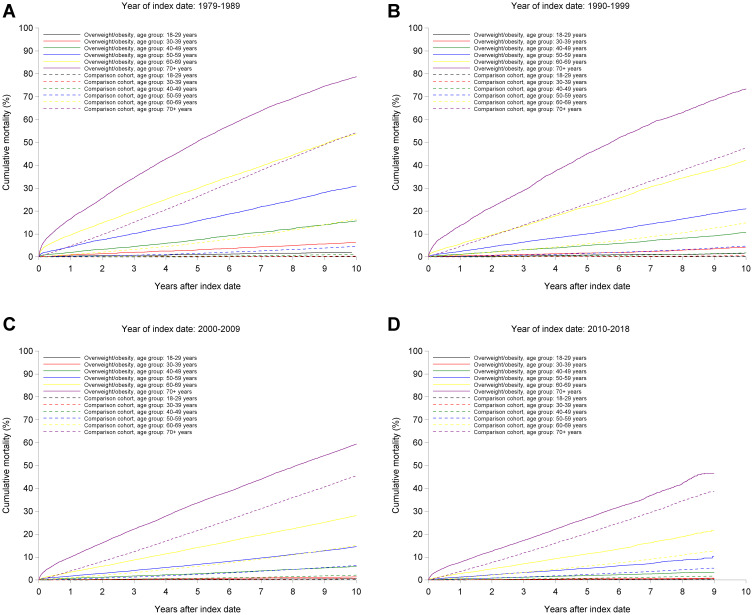
The overall aMRR was 1.70 (95% CI: 1.68-1.72) for patients with overweight/obesity, mainly due to diabetes and other endocrine diseases (aMRR=2.68 [95% CI: 2.57-2.81]), cardiovascular (aMRR=1.95 [95% CI: 1.91-1.98]), and respiratory diseases (aMRR=1.83 [95% CI: 1.77-1.89]). The 1-10-year aMRR decreased from 2.06 (95% CI: 2.01-2.11) in 1979-1989 to 1.29 (95% CI: 1.26-1.32) in 2000-2009. We found effect modification by age: age 18 to <30 years: aMRR=2.44 (95% CI: 2.24-2.66) vs age ≥70 years: 1.35 (95% CI: 1.33-1.37); comorbidities: baseline comorbidities: aMRR=1.13 (95% CI: 1.10-1.15) vs no comorbidities: aMRR=1.83 (95% CI: 1.80-1.85); and educational level: high educational level: aMRR=1.81 (95% CI: 1.74-1.88) vs low educational level: aMRR=1.70 (95% CI: 1.67-1.72).
Patients with overweight/obesity had a substantially increased long-term mortality, mainly due to diabetes, cardiovascular, and respiratory diseases. The excess mortality decreased during recent decades. Age, comorbidities, and socioeconomic factors modified the association.
关于医院诊断为超重/肥胖患者的长期死亡率数据有限。因此,我们旨在研究医院诊断为超重/肥胖患者的40年死亡率,包括特定病因死亡、长期时间趋势以及年龄、合并症和社会经济因素的潜在效应修正。
我们从国家登记处识别出1979年至2018年首次在医院诊断为超重/肥胖的所有丹麦人(N = 331,185),并构建了一个年龄和性别匹配的一般人群对照队列(N = 1,655,925)。我们计算了每1000人年的死亡率(MRs)以及调整后的死亡率比值(aMRRs)和95%置信区间(CIs),使用Cox回归并对合并症和教育水平进行调整。我们对年龄、合并症和社会经济因素进行了分层分析。
超重/肥胖患者的总体aMRR为1.70(95%CI:1.68 - 1.72),主要归因于糖尿病和其他内分泌疾病(aMRR = 2.68 [95%CI:2.57 - 2.81])、心血管疾病(aMRR = 1.95 [95%CI:1.91 - 1.98])和呼吸系统疾病(aMRR = 1.83 [95%CI:1.77 - 1.89])。1979 - 1989年期间1 - 10年的aMRR从2.06(95%CI:2.01 - 2.11)降至2000 - 2009年的1.29(95%CI:1.26 - 1.32)。我们发现年龄存在效应修正:18至<30岁:aMRR = 2.44(95%CI:2.24 - 2.66),而≥70岁:1.35(95%CI:1.33 - 1.37);合并症:基线合并症:aMRR = 1.13(95%CI:1.10 - 1.15),无合并症:aMRR = 1.83(95%CI:1.80 - 1.85);以及教育水平:高教育水平:aMRR = 1.81(95%CI:1.74 - 1.88),低教育水平:aMRR = 1.70(95%CI:1.67 - 1.72)。
超重/肥胖患者的长期死亡率大幅增加,主要归因于糖尿病、心血管疾病和呼吸系统疾病。近几十年来,额外死亡率有所下降。年龄、合并症和社会经济因素改变了这种关联。