Oral and Maxillofacial Diseases, University of Helsinki and Helsinki University Hospital, Helsinki, Finland.
Institute of Dentistry, University of Eastern Finland, Kuopio, Finland.
J Periodontol. 2022 Nov;93(11):1626-1634. doi: 10.1002/JPER.22-0005. Epub 2022 May 4.
In our recent genome-wide association study, we found that genetic polymorphisms in the complement factor H (CFH) gene and S100A gene region are strongly associated with serum matrix metalloproteinase 8 (MMP-8) concentration and the release of MMP-8 from neutrophils. As MMP-8 is centrally involved in the pathogenesis of periodontitis, we aimed to evaluate the presence of genetic polymorphisms of S100A8/A9/A12, MMP8, and CFH in periodontitis. In addition, we studied whether polymorphisms of these genes affect the concentrations of S100A8, S100A12, MMP-8, or complement activation marker in saliva.
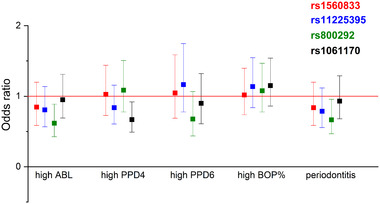
We genotyped four single-nucleotide polymorphisms (SNPs, rs1560833 in S100A8/A9/A12, rs11225395 in MMP8, rs800292 in CFH, and rs1061170 in CFH) and measured salivary concentrations of S100A8, S100A12, MMP-8, and terminal complement complex (TCC) in the Parogene cohort (n = 508). The cohort was composed of patients with an indication to coronary angiography and all underwent a clinical and radiographic oral examination.
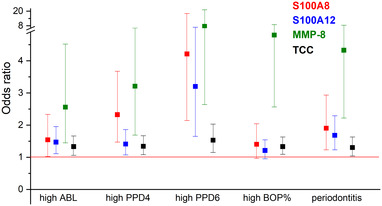
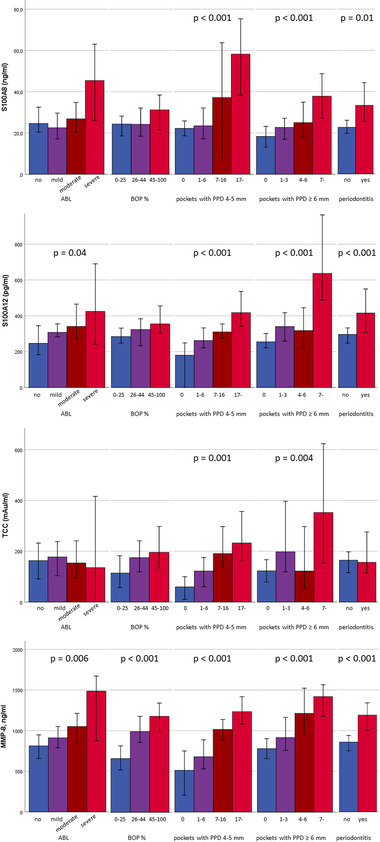
CFH polymorphisms rs800292 and rs1061170 were associated with periodontal parameters. None of the polymorphisms showed association with salivary proteins. However, salivary concentrations of S100A8, S100A12, MMP-8, and TCC were strongly associated with the number of periodontal pockets and alveolar bone loss.
Interestingly, genetic variants of CFH, MMP8, and S100A8/A9/A12 gene regions did not affect salivary levels of measured proteins. However, saliva levels of S100A8, S100A12, MMP-8, and TCC, and CFH polymorphisms were associated with clinical and radiographic signs of periodontitis. Our study further supports the observations that any dysregulation of complement may increase the risk of inflammatory disorders, such as periodontitis.
在我们最近的全基因组关联研究中,我们发现补体因子 H(CFH)基因和 S100A 基因区域的遗传多态性与血清基质金属蛋白酶 8(MMP-8)浓度以及中性粒细胞中 MMP-8 的释放密切相关。由于 MMP-8 是牙周炎发病机制中的核心因素,我们旨在评估牙周炎患者 S100A8/A9/A12、MMP8 和 CFH 基因的遗传多态性是否存在。此外,我们还研究了这些基因的多态性是否会影响唾液中 S100A8、S100A12、MMP-8 或补体激活标志物的浓度。
我们对四个单核苷酸多态性(SNP,S100A8/A9/A12 中的 rs1560833、MMP8 中的 rs11225395、CFH 中的 rs800292 和 CFH 中的 rs1061170)进行基因分型,并测量了 Parogene 队列(n=508)中唾液中的 S100A8、S100A12、MMP-8 和末端补体复合物(TCC)的浓度。该队列由有冠状动脉造影适应证的患者组成,所有患者均接受了临床和影像学口腔检查。
CFH 多态性 rs800292 和 rs1061170 与牙周参数相关。没有一个多态性与唾液蛋白有关。然而,S100A8、S100A12、MMP-8 和 TCC 的唾液浓度与牙周袋数量和牙槽骨丧失强烈相关。
有趣的是,CFH、MMP8 和 S100A8/A9/A12 基因区域的遗传变异并未影响测量蛋白的唾液水平。然而,S100A8、S100A12、MMP-8 和 TCC 的唾液水平以及 CFH 多态性与牙周炎的临床和影像学表现有关。我们的研究进一步支持这样的观点,即任何补体失调都可能增加炎症性疾病(如牙周炎)的风险。