The Wolfson Centre for Personalised Medicine, MRC Centre for Drug Safety Science, Department of Pharmacology and Therapeutics, Institute of Systems, Molecular and Integrative Biology, University of Liverpool, Liverpool, UK.
Department of Health Data Science, Institute of Population Health Sciences, University of Liverpool, United Kingdom Institute of Population Health Sciences, University of Liverpool, Liverpool, UK.
Br J Clin Pharmacol. 2022 Aug;88(8):3577-3599. doi: 10.1111/bcp.15331. Epub 2022 Apr 25.
To update our previously reported systematic review and meta-analysis of observational studies on cardiovascular drug exposure and COVID-19 clinical outcomes by focusing on newly published randomized controlled trials (RCTs).
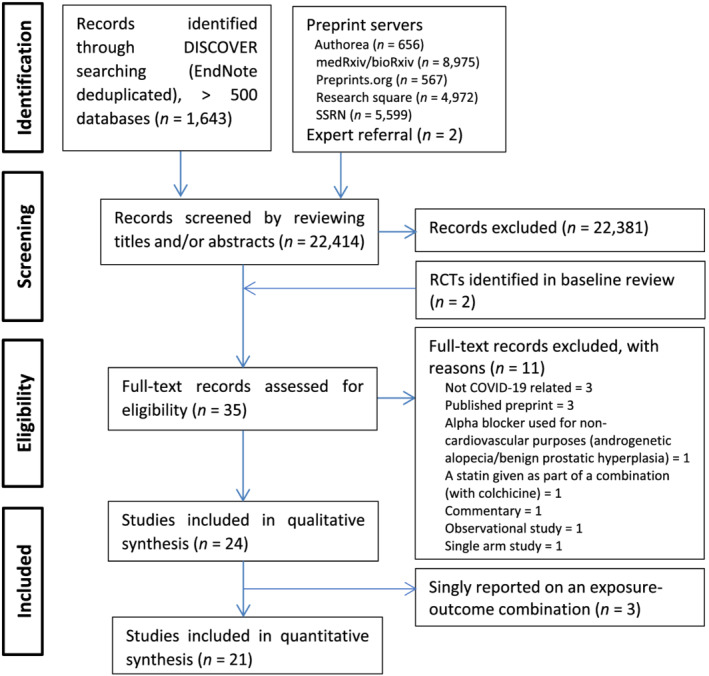
More than 500 databases were searched between 1 November 2020 and 2 October 2021 to identify RCTs that were published after our baseline review. One reviewer extracted data with other reviewers verifying the extracted data for accuracy and completeness.
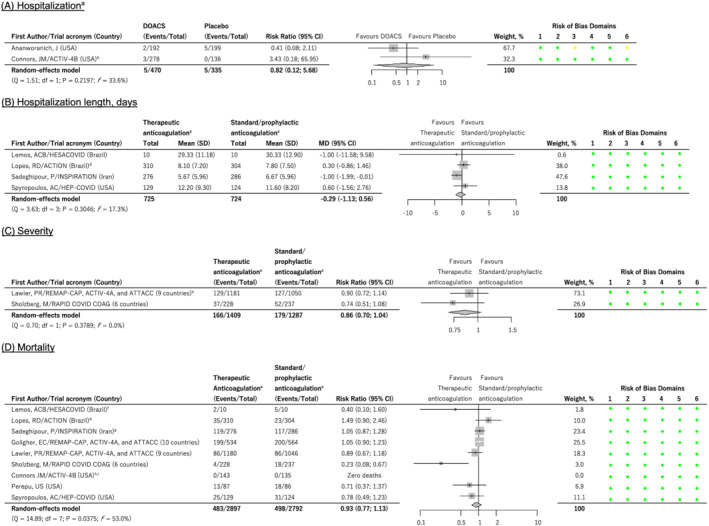
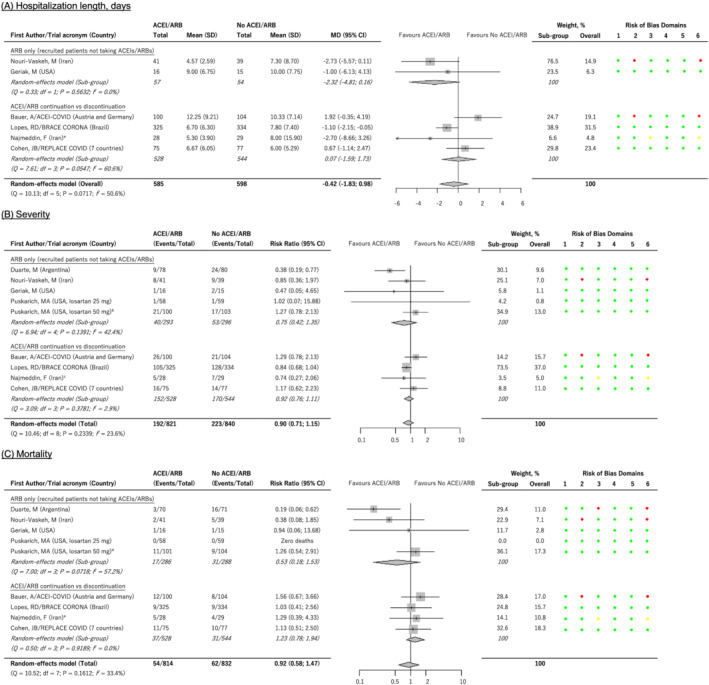
After screening 22 414 records, we included 24 and 21 RCTs in the qualitative and quantitative syntheses, respectively. The most investigated drug classes were angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blocker (ARBs) and anticoagulants, investigated by 10 and 11 studies respectively. In meta-analyses, ACEI/ARBs did not affect hospitalization length (mean difference -0.42, 95% confidence interval [CI] -1.83; 0.98 d, n = 1183), COVID-19 severity (risk ratio/RR 0.90, 95% CI 0.71; 1.15, n = 1661) or mortality (risk ratio [RR] 0.92, 95% CI 0.58; 1.47, n = 1646). Therapeutic anticoagulation also had no effect (hospitalization length mean difference -0.29, 95% CI -1.13 to 0.56 d, n = 1449; severity RR 0.86, 95% CI 0.70; 1.04, n = 2696; and, mortality RR 0.93, 95% CI 0.77; 1.13, n = 5689). Other investigated drug classes were antiplatelets (aspirin, 2 trials), antithrombotics (sulodexide, 1 trial), calcium channel blockers (amlodipine, 1 trial) and lipid-modifying drugs (atorvastatin, 1 trial).
Moderate- to high-certainty RCT evidence suggests that cardiovascular drugs such as ACEIs/ARBs are not associated with poor COVID-19 outcomes, and should therefore not be discontinued. These cardiovascular drugs should also not be initiated to treat or prevent COVID-19 unless they are needed for an underlying currently approved therapeutic indication.
通过关注新发表的随机对照试验(RCT),更新我们之前关于心血管药物暴露与 COVID-19 临床结局的观察性研究的系统评价和荟萃分析。
在 2020 年 11 月 1 日至 2021 年 10 月 2 日期间,我们对 500 多个数据库进行了搜索,以确定在我们的基线审查后发表的 RCT。一位审查员提取数据,其他审查员验证提取数据的准确性和完整性。
在筛选了 22414 条记录后,我们分别将 24 项和 21 项 RCT 纳入定性和定量综合分析。研究最多的药物类别是血管紧张素转换酶抑制剂(ACEI)/血管紧张素受体阻滞剂(ARB)和抗凝剂,分别有 10 项和 11 项研究对其进行了研究。在荟萃分析中,ACEI/ARB 并未影响住院时间(平均差异-0.42,95%置信区间[CI]-1.83;0.98 d,n=1183)、COVID-19 严重程度(风险比[RR]0.90,95%CI 0.71;1.15,n=1661)或死亡率(风险比[RR]0.92,95%CI 0.58;1.47,n=1646)。治疗性抗凝也没有效果(住院时间平均差异-0.29,95%CI-1.13 至 0.56 d,n=1449;严重程度 RR 0.86,95%CI 0.70;1.04,n=2696;死亡率 RR 0.93,95%CI 0.77;1.13,n=5689)。其他研究的药物类别包括抗血小板药物(阿司匹林,2 项试验)、抗血栓药物(舒洛地特,1 项试验)、钙通道阻滞剂(氨氯地平,1 项试验)和调脂药物(阿托伐他汀,1 项试验)。
中至高度确定性 RCT 证据表明,心血管药物如 ACEI/ARB 与 COVID-19 不良结局无关,因此不应停药。除非这些药物是治疗或预防潜在目前批准的治疗适应证所必需的,否则不应启动这些心血管药物来治疗或预防 COVID-19。