Infectious Diseases Unit, Hospital Universitario Reina Sofía-Instituto Maimónides de Investigación Biomédica de Córdoba (IMIBIC)-Universidad de Córdoba, Córdoba, Spain.
Centro de Investigación Biomédica en Red en Enfermedades Infecciosas (CIBERINFEC), Instituto de Salud Carlos III, Seville, Spain.
Microbiol Spectr. 2022 Apr 27;10(2):e0197021. doi: 10.1128/spectrum.01970-21. Epub 2022 Mar 24.
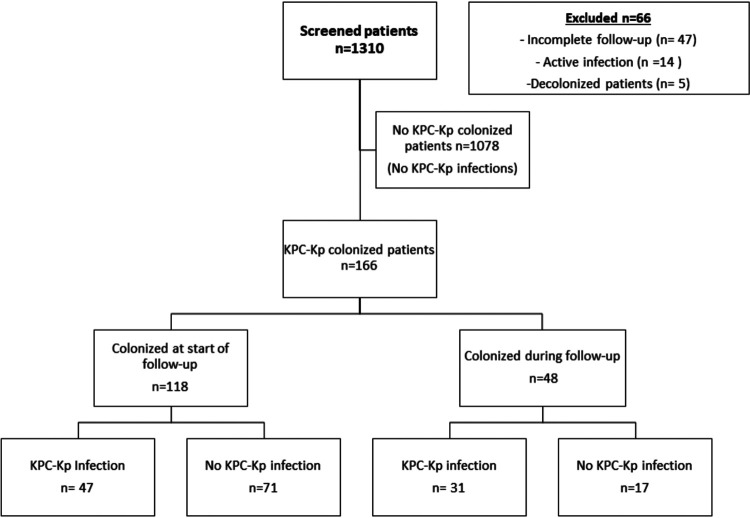
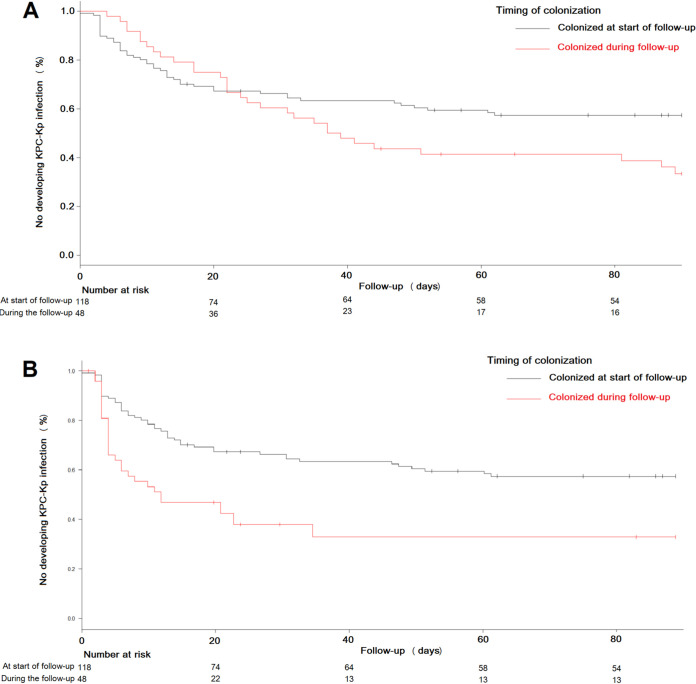
Colonization by KPC-producing Klebsiella pneumoniae (KPC-Kp) is associated with the risk of developing KPC-Kp infection. The impact of the time elapsed since a patient becomes colonized on this risk is not well known. An observational, prospective, longitudinal cohort study of colonized patients undergoing active rectal culture screening to rule out KPC-Kp colonization (July 2012 to November 2017). Patients with a positive culture at inclusion (colonized at start of follow-up) and those with a negative culture at inclusion who became colonized within 90 days (colonized during follow-up) were included in the analysis. CART analysis was used to dichotomize variables according to their association with infection. Kaplan-Meier infection-free survival curves and the log-rank test were used for group comparisons. Logistic regression was used to identify variables associated with KPC-Kp infection. Among 1310 patients included, 166 were colonized at the end of follow-up. Forty-seven out of 118 patients colonized at start of follow-up developed infection (39.8%) versus 31 out of 48 patients colonized during follow-up (64.6%; = 0.006). Variables associated with KPC-Kp infection in the logistic regression analysis were: colonization detection during follow-up (OR, 2.74; 95% CI, 1.07 to 7.04; = 0.03), Giannella risk score (OR, 1.51; 95% CI, 1.32 to 1.73; < 0.001), high-risk ward (OR, 4.77; 95% CI, 1.61 to 14.10; = 0.005) and urological manipulation after admission (OR, 3.69; 95% CI, 1.08 to 12.60; = 0.04). In 25 out of 31 patients (80.6%) colonized during follow-up who developed KPC-Kp infection, infection appeared within 15 days after colonization. The risk of KPC-Kp infection was higher when colonization is recently acquired during hospitalization. In this prospective study, we concluded that the timing of colonization was a factor to assess when considering empirical treatment for suspected KPC-Kp infection and prophylaxis or infection control. In this study, it was confirmed that patients who became colonized during hospitalization had a higher risk of developing KPC-Kp infection than hospitalized patients who were already colonized at the start of follow-up. Besides, the risk of infection in the group of patients who became colonized during follow-up was greater in the first weeks immediately after colonization was confirmed. Our findings support the need for designing preventive strategies for patients at the highest risk of infection development, including those admitted in high-risk hospital wards and those undergoing urological procedures.
产碳青霉烯酶肺炎克雷伯菌(KPC-Kp)定植与 KPC-Kp 感染风险相关。患者定植后时间对该风险的影响尚不清楚。这是一项对接受主动直肠培养筛查以排除 KPC-Kp 定植的定植患者进行的观察性、前瞻性、纵向队列研究(2012 年 7 月至 2017 年 11 月)。纳入标准为:纳入时培养阳性(定植于随访开始时)和纳入时培养阴性但在 90 天内定植(定植于随访期间)的患者。CART 分析用于根据与感染相关的关联将变量分为两类。Kaplan-Meier 无感染生存曲线和对数秩检验用于组间比较。Logistic 回归用于确定与 KPC-Kp 感染相关的变量。在纳入的 1310 例患者中,166 例在随访结束时定植。在随访开始时定植的 118 例患者中有 47 例发生感染(39.8%),而在随访期间定植的 48 例患者中有 31 例发生感染(64.6%; = 0.006)。Logistic 回归分析中与 KPC-Kp 感染相关的变量包括:随访期间的定植检测(OR,2.74;95%CI,1.07 至 7.04; = 0.03)、Giannella 风险评分(OR,1.51;95%CI,1.32 至 1.73; < 0.001)、高危病房(OR,4.77;95%CI,1.61 至 14.10; = 0.005)和入院后泌尿科操作(OR,3.69;95%CI,1.08 至 12.60; = 0.04)。在 31 例定植期间发生 KPC-Kp 感染的患者中,有 25 例(80.6%)在定植后 15 天内出现感染。住院期间近期定植时,KPC-Kp 感染的风险更高。在这项前瞻性研究中,我们得出结论,定植时间是考虑疑似 KPC-Kp 感染的经验性治疗和预防或感染控制时需要评估的因素。在这项研究中,我们证实了与定植于随访开始时的住院患者相比,住院期间定植的患者发生 KPC-Kp 感染的风险更高。此外,在随访期间定植的患者中,在定植后立即确认后的最初几周内,感染的风险更大。我们的研究结果支持为感染发展风险最高的患者制定预防策略,包括入住高危病房的患者和接受泌尿科手术的患者。