Cambodia Oxford Medical Research Unit, Angkor Hospital for Children, Siem Reap, Cambodia.
Centre for Tropical Medicine & Global Health, University of Oxford, Oxford, United Kingdom.
Clin Infect Dis. 2022 Aug 24;75(1):e368-e379. doi: 10.1093/cid/ciac224.
In locations where few people have received coronavirus disease 2019 (COVID-19) vaccines, health systems remain vulnerable to surges in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections. Tools to identify patients suitable for community-based management are urgently needed.
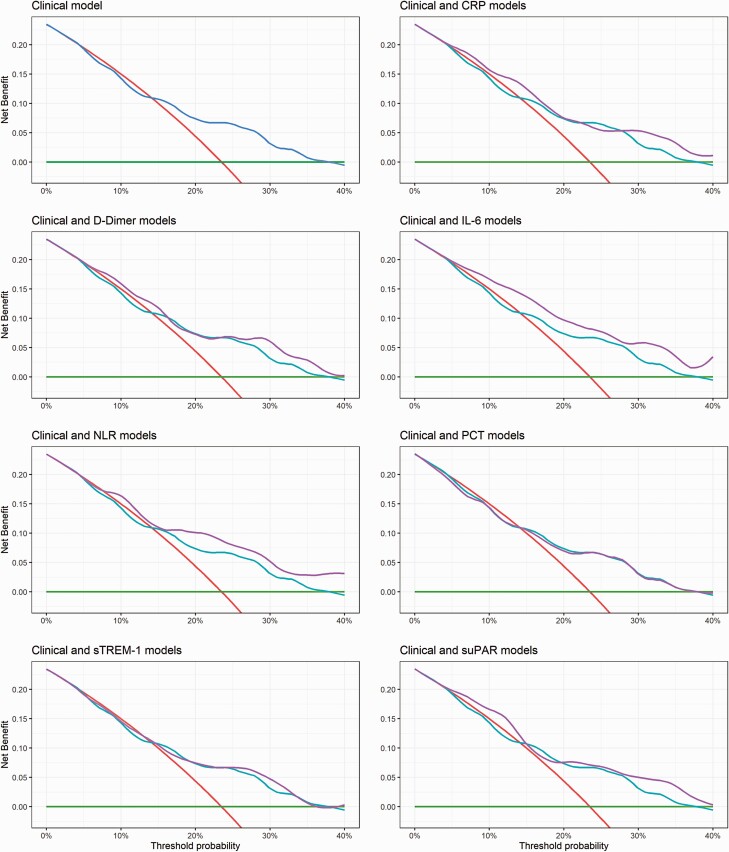
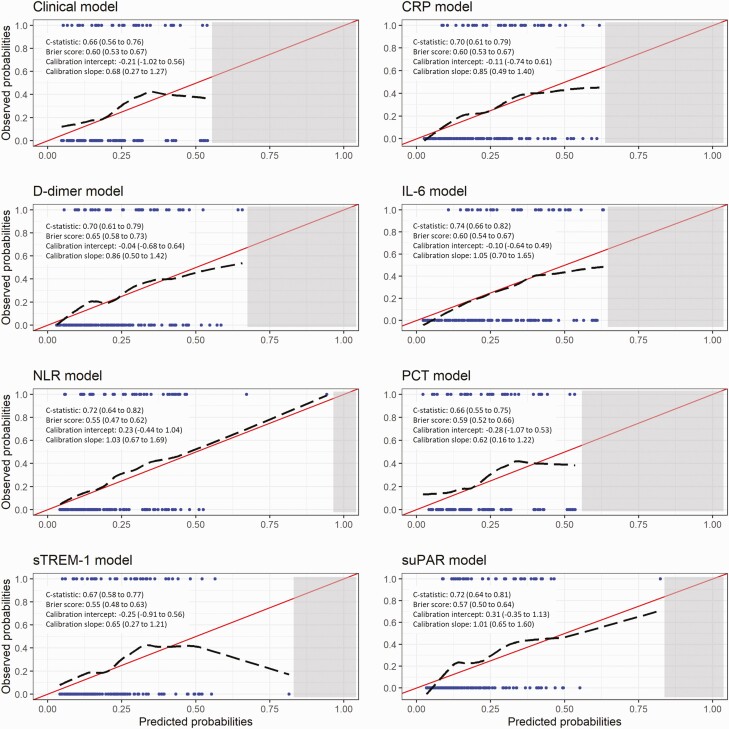
We prospectively recruited adults presenting to 2 hospitals in India with moderate symptoms of laboratory-confirmed COVID-19 to develop and validate a clinical prediction model to rule out progression to supplemental oxygen requirement. The primary outcome was defined as any of the following: SpO2 < 94%; respiratory rate > 30 BPM; SpO2/FiO2 < 400; or death. We specified a priori that each model would contain three clinical parameters (age, sex, and SpO2) and 1 of 7 shortlisted biochemical biomarkers measurable using commercially available rapid tests (C-reactive protein [CRP], D-dimer, interleukin 6 [IL-6], neutrophil-to-lymphocyte ratio [NLR], procalcitonin [PCT], soluble triggering receptor expressed on myeloid cell-1 [sTREM-1], or soluble urokinase plasminogen activator receptor [suPAR]), to ensure the models would be suitable for resource-limited settings. We evaluated discrimination, calibration, and clinical utility of the models in a held-out temporal external validation cohort.
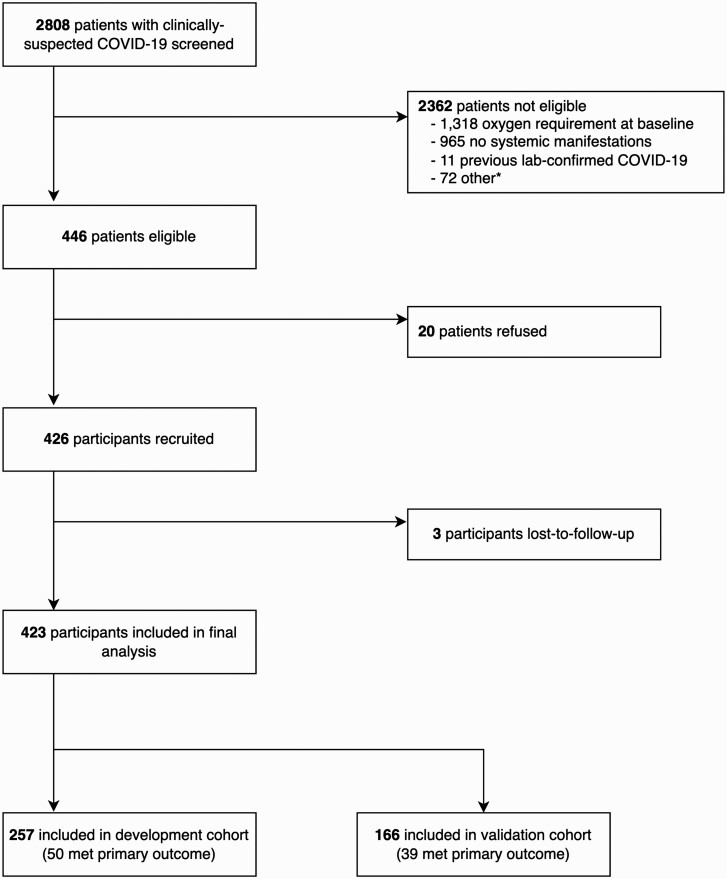
In total, 426 participants were recruited, of whom 89 (21.0%) met the primary outcome; 257 participants comprised the development cohort, and 166 comprised the validation cohort. The 3 models containing NLR, suPAR, or IL-6 demonstrated promising discrimination (c-statistics: 0.72-0.74) and calibration (calibration slopes: 1.01-1.05) in the validation cohort and provided greater utility than a model containing the clinical parameters alone.
We present 3 clinical prediction models that could help clinicians identify patients with moderate COVID-19 suitable for community-based management. The models are readily implementable and of particular relevance for locations with limited resources.
在很少有人接种 2019 年冠状病毒病(COVID-19)疫苗的地方,卫生系统仍然容易受到严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染的冲击。迫切需要找到识别适合社区管理的患者的工具。
我们前瞻性地招募了在印度 2 家医院就诊的患有中度实验室确诊 COVID-19 症状的成年人,以开发和验证一种临床预测模型,以排除进展为补充氧气需求的可能性。主要结局定义为以下任何一种情况:SpO2<94%;呼吸频率>30 次/分;SpO2/FiO2<400;或死亡。我们预先规定,每个模型将包含三个临床参数(年龄、性别和 SpO2)和 7 个经筛选的生物化学标志物中的 1 个,这些标志物可以使用市售的快速检测(C 反应蛋白[CRP]、D-二聚体、白细胞介素 6[IL-6]、中性粒细胞与淋巴细胞比值[NLR]、降钙素原[PCT]、髓系细胞表达的触发受体 1[soluble triggering receptor expressed on myeloid cell-1,sTREM-1]或可溶性尿激酶型纤溶酶原激活物受体[soluble urokinase plasminogen activator receptor,suPAR]),以确保模型适用于资源有限的环境。我们在一个时间外验证队列中评估了模型的区分度、校准度和临床实用性。
共有 426 名参与者入组,其中 89 名(21.0%)达到主要结局;257 名参与者构成开发队列,166 名参与者构成验证队列。包含 NLR、suPAR 或 IL-6 的 3 个模型在验证队列中表现出有前景的区分度(C 统计量:0.72-0.74)和校准(校准斜率:1.01-1.05),并且比仅包含临床参数的模型具有更大的实用性。
我们提出了 3 种临床预测模型,可帮助临床医生识别适合社区管理的中度 COVID-19 患者。这些模型易于实施,对于资源有限的地区具有特别重要的意义。