Garinet Simon, Wang Pascal, Mansuet-Lupo Audrey, Fournel Ludovic, Wislez Marie, Blons Hélène
Pharmacogenomics and Molecular Oncology Unit, Biochemistry Department, Assistance Publique-Hopitaux de Paris, Hôpital Européen Georges Pompidou, 75015 Paris, France.
Centre de Recherche des Cordeliers, INSERM UMRS-1138, Sorbonne Université, Université de Paris, 75006 Paris, France.
Cancers (Basel). 2022 Mar 9;14(6):1400. doi: 10.3390/cancers14061400.
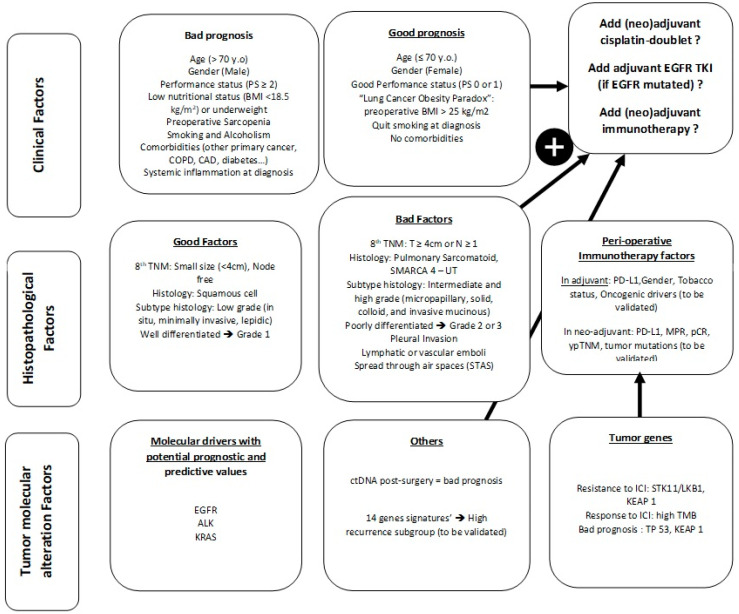
Lung cancer is the most common cause of cancer mortality worldwide, and non-small cell lung cancer (NSCLC) represents 80% of lung cancer subtypes. Patients with localized non-small cell lung cancer may be considered for upfront surgical treatment. However, the overall 5-year survival rate is 59%. To improve survival, adjuvant chemotherapy (ACT) was largely explored and showed an overall benefit of survival at 5 years < 7%. The evaluation of recurrence risk and subsequent need for ACT is only based on tumor stage (TNM classification); however, more than 25% of patients with stage IA/B tumors will relapse. Recently, adjuvant targeted therapy has been approved for EGFR-mutated resected NSCLC and trials are evaluating other targeted therapies and immunotherapies in adjuvant settings. Costs, treatment duration, emergence of resistant clones and side effects stress the need for a better selection of patients. The identification and validation of prognostic and theranostic markers to better stratify patients who could benefit from adjuvant therapies are needed. In this review, we report current validated clinical, pathological and molecular prognosis biomarkers that influence outcome in resected NSCLC, and we also describe molecular biomarkers under evaluation that could be available in daily practice to drive ACT in resected NSCLC.
肺癌是全球癌症死亡的最常见原因,非小细胞肺癌(NSCLC)占肺癌亚型的80%。局限性非小细胞肺癌患者可考虑进行 upfront 手术治疗。然而,总体5年生存率为59%。为了提高生存率,人们对辅助化疗(ACT)进行了大量探索,结果显示5年生存率的总体获益<7%。复发风险评估及后续ACT需求仅基于肿瘤分期(TNM分类);然而,超过25%的IA/B期肿瘤患者会复发。最近,辅助靶向治疗已被批准用于EGFR突变的可切除NSCLC,并且正在进行试验以评估辅助治疗中的其他靶向治疗和免疫治疗。成本、治疗持续时间、耐药克隆的出现以及副作用凸显了更好地选择患者的必要性。需要识别和验证预后及诊疗标志物,以便更好地对可能从辅助治疗中获益的患者进行分层。在本综述中,我们报告了目前已验证的影响可切除NSCLC预后的临床、病理和分子预后生物标志物,并且我们还描述了正在评估的分子生物标志物,这些标志物在日常实践中可能有助于指导可切除NSCLC的ACT。