Chai Yue, Wu Xinyu, Bai Hua, Duan Jianchun
Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China.
J Clin Med. 2022 Mar 16;11(6):1655. doi: 10.3390/jcm11061655.
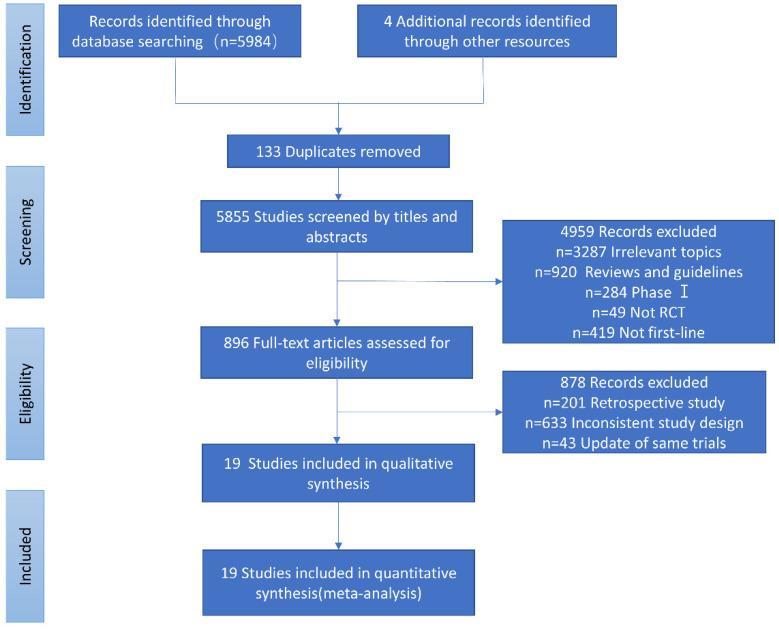
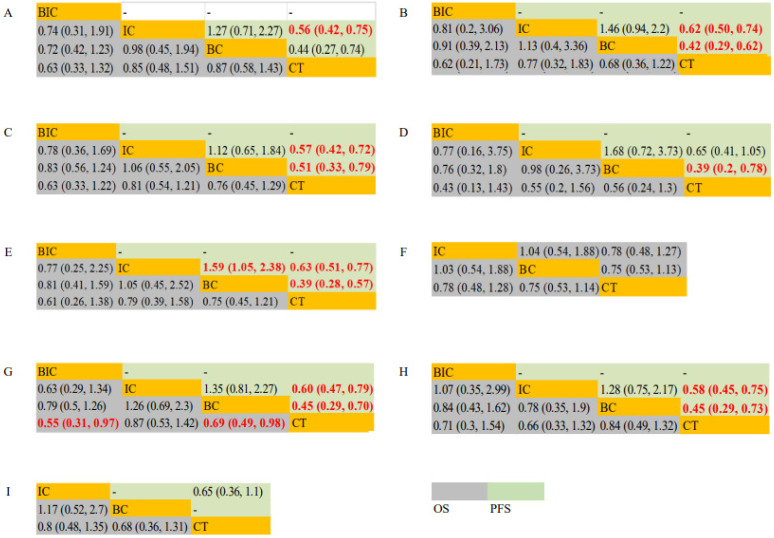
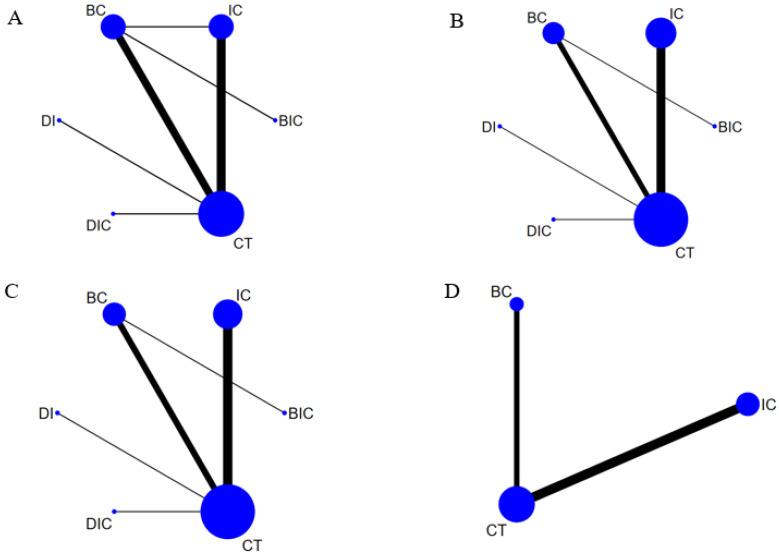
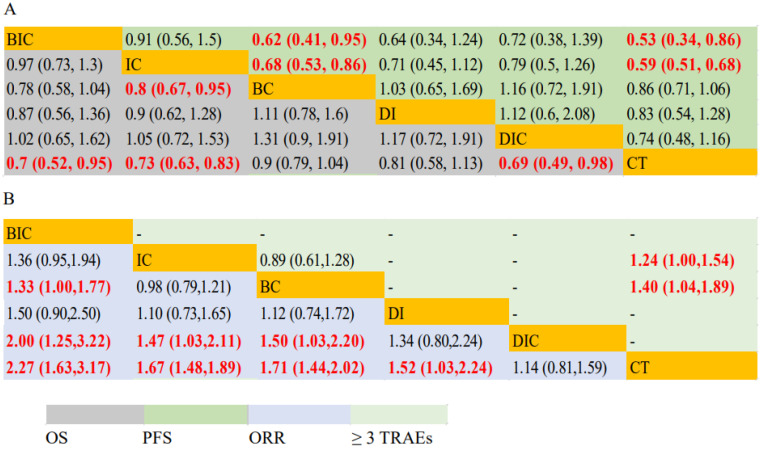
Background: A network meta-analysis was conducted to summarize randomized control trials and updated results to evaluate the efficacy and safety profiles of existing first-line therapies for advanced non-squamous non-small cell lung cancer (NSCLC) patients without known driver gene mutations. Patients and Methods: Eligible studies were identified following a systematic search of the Cochrane Library, PubMed, Embase, Web of Science, Wanfang Data, and the China Knowledge Resource Integrated Database from January 2000 to December 2021. Results: Nineteen trials involving 8176 patients with driver-gene-negative advanced non-squamous NSCLC were included. For patients with driver-gene-negative advanced NSCLC, immunotherapy + chemotherapy (IC) significantly prolonged overall survival (OS) (hazard ratio (HR), 0.80; 95% confidence intervals (CI): 0.67−0.95) and progression-free survival (PFS) (HR, 0.68; 95% CI: 0.53−0.86) compared with bevacizumab + chemotherapy (BC), with a similar objective response rate and incidence of ≥3 treatment-related adverse events (TRAEs) (risk ratios (RR), 0.98; 95% CI: 0.79−1.21/RR, 0.89; 95% CI: 0.61−1.28; respectively) compared with BC. IC yielded a superior PFS rate (HR, 1.59; 95% CI: 1.05−2.38) compared to BC in the subgroup of patients < 65 years old. Conclusions: Currently, IC is a more efficient first-line therapy for driver-gene-negative advanced non-squamous NSCLC patients, with prolonged PFS and OS, as well as a comparatively lower risk of ≥3 TRAEs compared to BC.
进行了一项网状Meta分析,以总结随机对照试验及更新结果,评估现有一线治疗方案对无已知驱动基因突变的晚期非鳞状非小细胞肺癌(NSCLC)患者的疗效和安全性。
通过系统检索Cochrane图书馆、PubMed、Embase、Web of Science、万方数据和中国知网,确定2000年1月至2021年12月期间的合格研究。
纳入了19项试验,共8176例驱动基因阴性的晚期非鳞状NSCLC患者。对于驱动基因阴性的晚期NSCLC患者,与贝伐单抗联合化疗(BC)相比,免疫治疗联合化疗(IC)显著延长了总生存期(OS)(风险比(HR),0.80;95%置信区间(CI):0.67−0.95)和无进展生存期(PFS)(HR,0.68;95%CI:0.53−0.86),客观缓解率和≥3级治疗相关不良事件(TRAEs)发生率与BC相似(风险比(RR)分别为0.98;95%CI:0.79−1.21/RR,0.89;95%CI:0.61−1.28)。在年龄<65岁的患者亚组中,IC与BC相比PFS率更高(HR,1.59;95%CI:1.05−2.38)。
目前,对于驱动基因阴性的晚期非鳞状NSCLC患者,IC是一种更有效的一线治疗方案,与BC相比,可延长PFS和OS,且≥3级TRAEs风险相对较低。