Pelosi Paolo, Tonelli Roberto, Torregiani Chiara, Baratella Elisa, Confalonieri Marco, Battaglini Denise, Marchioni Alessandro, Confalonieri Paola, Clini Enrico, Salton Francesco, Ruaro Barbara
Anesthesia and Critical Care, San Martino Policlinico Hospital, IRCCS for Oncology and Neurosciences, 16132 Genoa, Italy.
Department of Surgical Sciences and Integrated Diagnostics, University of Genoa, 16132 Genoa, Italy.
J Clin Med. 2022 Mar 19;11(6):1704. doi: 10.3390/jcm11061704.
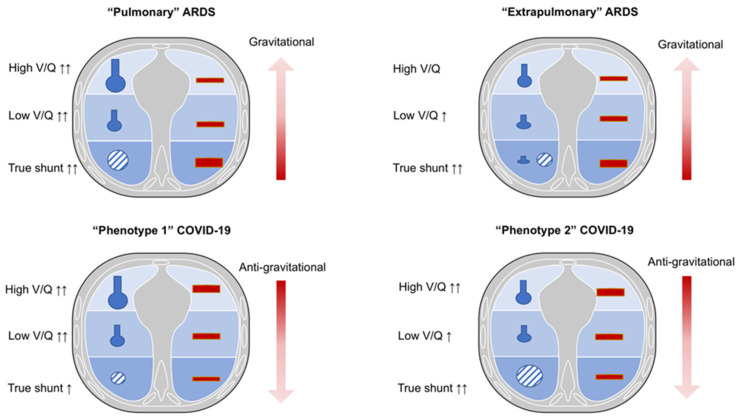
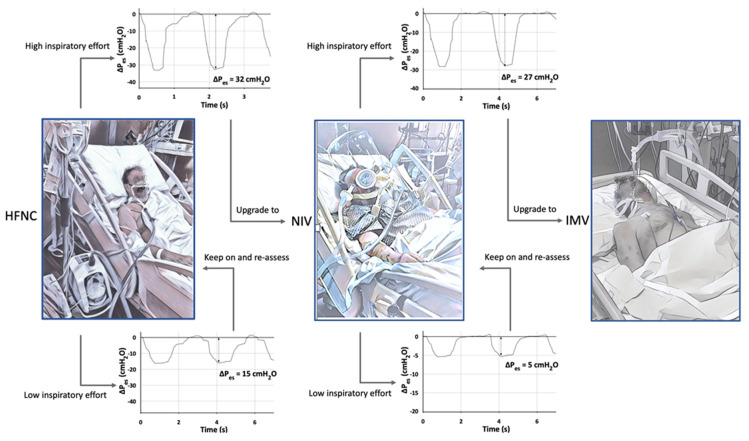
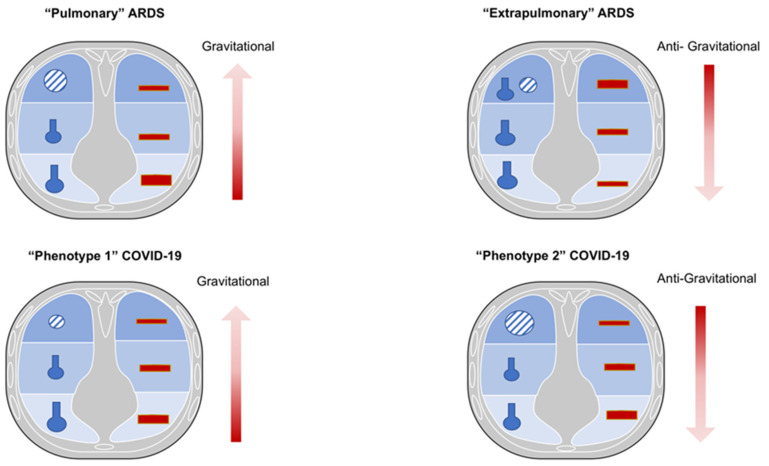
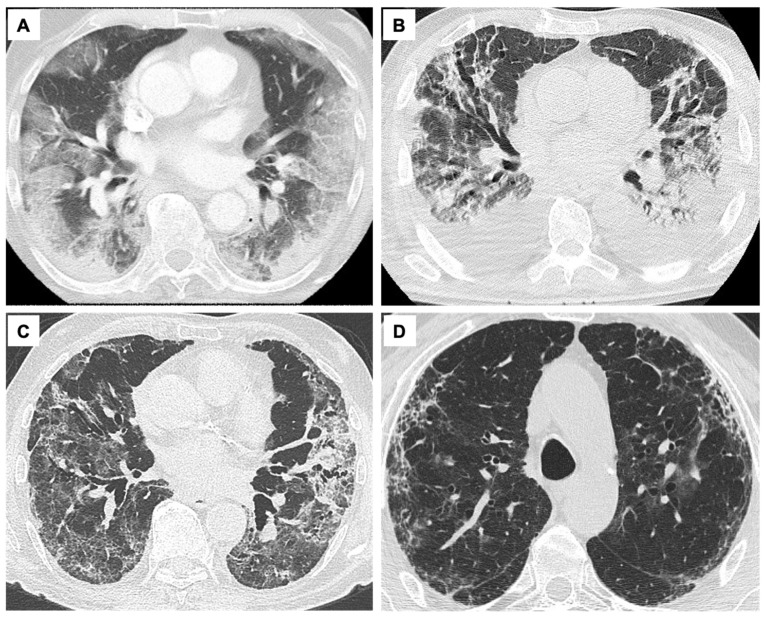
The latest guidelines for the hospital care of patients affected by coronavirus disease 2019 (COVID-19)-related acute respiratory failure have moved towards the widely accepted use of noninvasive respiratory support (NIRS) as opposed to early intubation at the pandemic onset. The establishment of severe COVID-19 pneumonia goes through different pathophysiological phases that partially resemble typical acute respiratory distress syndrome (ARDS) and have been categorized into different clinical-radiological phenotypes. These can variably benefit on the application of external positive end-expiratory pressure (PEEP) during noninvasive mechanical ventilation, mainly due to variable levels of lung recruitment ability and lung compliance during different phases of the disease. A growing body of evidence suggests that intense respiratory effort producing excessive negative pleural pressure swings (P) plays a critical role in the onset and progression of lung and diaphragm damage in patients treated with noninvasive respiratory support. Routine respiratory monitoring is mandatory to avoid the nasty continuation of NIRS in patients who are at higher risk for respiratory deterioration and could benefit from early initiation of invasive mechanical ventilation instead. Here we propose different monitoring methods both in the clinical and experimental settings adapted for this purpose, although further research is required to allow their extensive application in clinical practice. We reviewed the needs and available tools for clinical-physiological monitoring that aims at optimizing the ventilatory management of patients affected by acute respiratory distress syndrome due to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection.
2019冠状病毒病(COVID-19)相关急性呼吸衰竭患者的最新医院护理指南已倾向于广泛使用无创呼吸支持(NIRS),而非在疫情初期进行早期插管。重症COVID-19肺炎的发展经历不同的病理生理阶段,部分类似于典型的急性呼吸窘迫综合征(ARDS),并已被分类为不同的临床-放射学表型。这些表型在无创机械通气期间应用外部呼气末正压(PEEP)时可能会有不同程度的获益,主要是由于疾病不同阶段肺复张能力和肺顺应性水平不同。越来越多的证据表明,在接受无创呼吸支持治疗的患者中,产生过度胸膜负压波动(P)的强烈呼吸努力在肺和膈肌损伤的发生和发展中起关键作用。对于有呼吸恶化高风险且可能从早期有创机械通气中获益的患者,常规呼吸监测是必要的,以避免持续进行无创呼吸支持带来不良后果。尽管还需要进一步研究以使其能在临床实践中广泛应用,但我们在此提出适用于此目的的临床和实验环境中的不同监测方法。我们回顾了旨在优化由严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染引起的急性呼吸窘迫综合征患者通气管理的临床生理监测的需求和可用工具。