Hamel C C, Vart P, Vandenbussche F P H A, Braat D D M, Snijders M P L M, Coppus S F P J
Department of Obstetrics and Gynaecology, Radboud University Medical Centre, Nijmegen, the Netherlands.
Department of Obstetrics and Gynaecology, Canisius Wilhelmina Hospital, Nijmegen, the Netherlands.
Hum Reprod. 2022 May 3;37(5):936-946. doi: 10.1093/humrep/deac048.
What are clinical predictors for successful medical treatment in case of early pregnancy loss (EPL)?
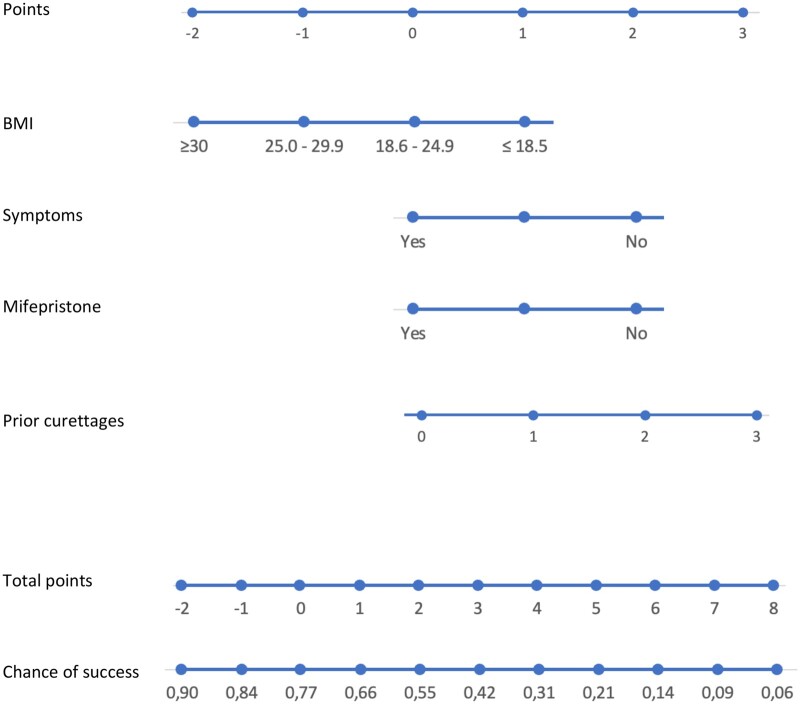
Use of mifepristone, BMI, number of previous uterine aspirations and the presence of minor clinical symptoms (slight vaginal bleeding or some abdominal cramps) at treatment start are predictors for successful medical treatment in case of EPL.
Success rates of medical treatment for EPL vary strongly, between but also within different treatment regimens. Up until now, although some predictors have been identified, no clinical prediction model has been developed yet.
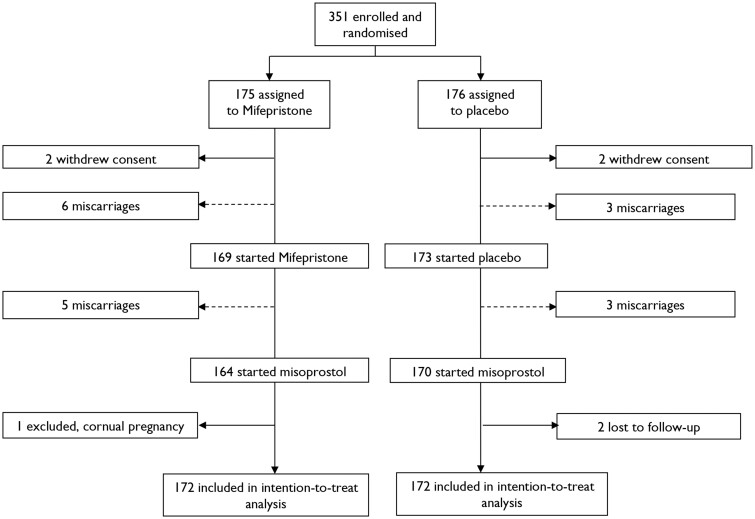
STUDY DESIGN, SIZE, DURATION: Secondary analysis of a multicentre randomized controlled trial in 17 Dutch hospitals, executed between 28 June 2018 and 8 January 2020.
PARTICIPANTS/MATERIALS, SETTING, METHODS: Women with a non-viable pregnancy between 6 and 14 weeks of gestational age, who opted for medical treatment after a minimum of 1 week of unsuccessful expectant management. Potential predictors for successful medical treatment of EPL were chosen based on literature and expert opinions. We internally validated the prediction model using bootstrapping techniques.
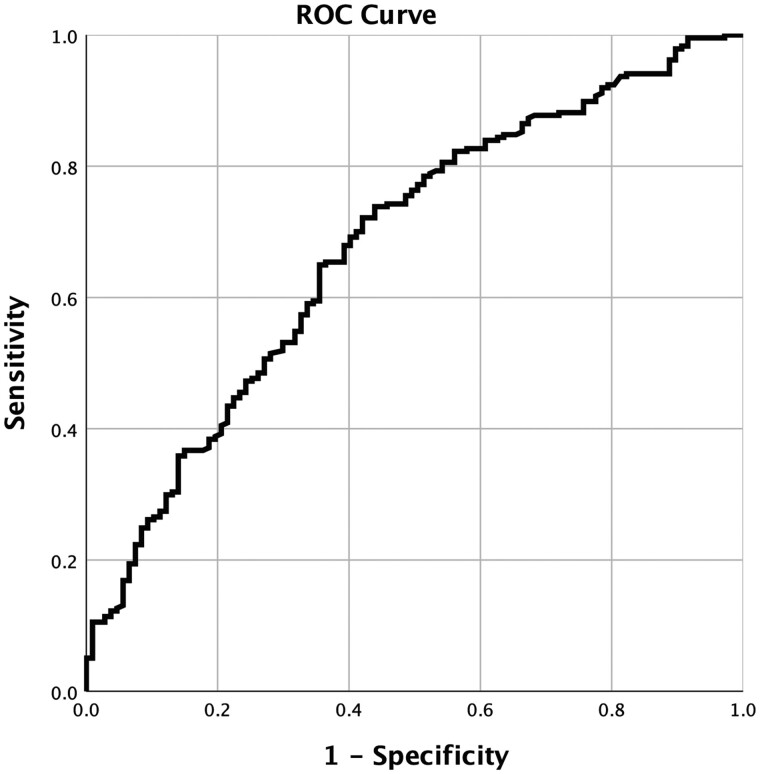
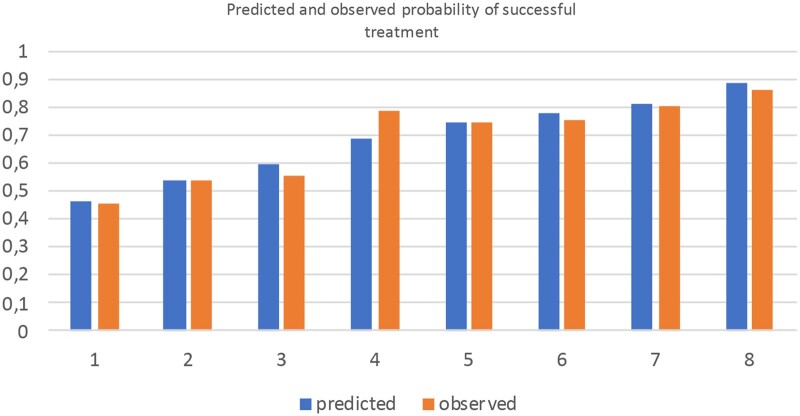
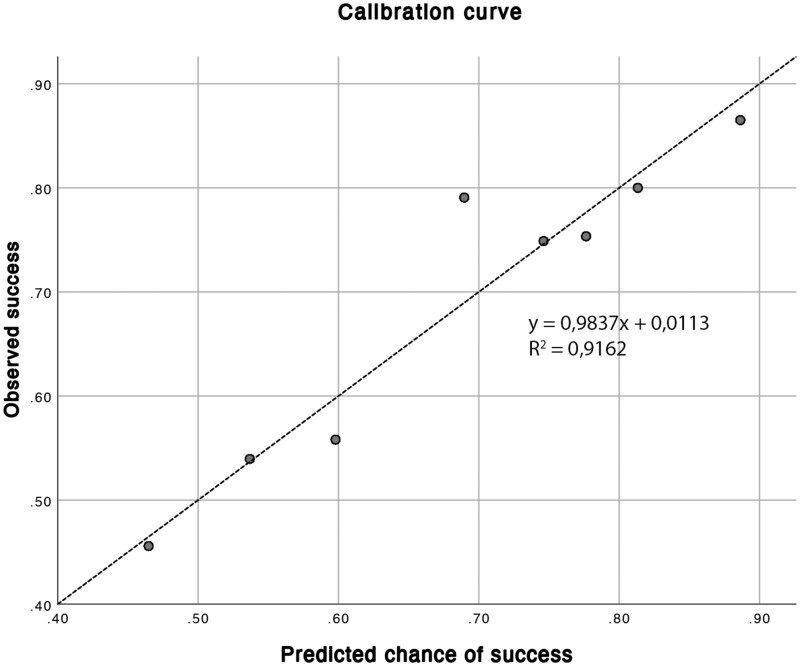
237 out of 344 women had a successful medical EPL treatment (68.9%). The model includes the following variables: use of mifepristone, BMI, number of previous uterine aspirations and the presence of minor clinical symptoms (slight vaginal bleeding or some abdominal cramps) at treatment start. The model shows a moderate capacity to discriminate between success and failure of treatment, with an AUC of 67.6% (95% CI = 64.9-70.3%). The model had a good fit comparing predicted to observed probabilities of success but might underestimate treatment success in women with a predicted probability of success of ∼70%.
LIMITATIONS, REASONS FOR CAUTION: The vast majority (90.4%) of women were Caucasian, potentially leading to less optimal model performance in a non-Caucasian population. Limitations of our model are that we have not yet been able to externally validate its performance and clinical impact, and the moderate accuracy of the prediction model of 0.67.
We developed a prediction model, aimed to improve and personalize counselling for medical treatment of EPL by providing a woman with her individual chance of complete evacuation.
STUDY FUNDING/COMPETING INTEREST(S): The Triple M Trial, upon which this secondary analysis was performed, was funded by the Healthcare Insurers Innovation Foundation (project number 3080 B15-191).
Clinicaltrials.gov: NCT03212352.
早期妊娠丢失(EPL)时药物治疗成功的临床预测因素有哪些?
米非司酮的使用、体重指数(BMI)、既往子宫吸刮术次数以及治疗开始时存在轻微临床症状(轻微阴道出血或一些腹部绞痛)是EPL时药物治疗成功的预测因素。
EPL药物治疗的成功率差异很大,不同治疗方案之间以及同一治疗方案内部均如此。到目前为止,虽然已经确定了一些预测因素,但尚未开发出临床预测模型。
研究设计、规模、持续时间:对17家荷兰医院进行的一项多中心随机对照试验的二次分析,该试验于2018年6月28日至2020年1月8日进行。
参与者/材料、设置、方法:孕周在6至14周之间的不可行妊娠妇女,在至少1周的期待管理失败后选择药物治疗。基于文献和专家意见选择EPL药物治疗成功的潜在预测因素。我们使用自抽样技术对预测模型进行了内部验证。
344名妇女中有237名药物治疗EPL成功(68.9%)。该模型包括以下变量:米非司酮的使用、BMI、既往子宫吸刮术次数以及治疗开始时存在轻微临床症状(轻微阴道出血或一些腹部绞痛)。该模型显示出区分治疗成功与失败的中等能力,曲线下面积(AUC)为67.6%(95%置信区间=64.9 - 70.3%)。与观察到的成功概率相比,该模型拟合良好,但可能会低估预测成功概率约70%的女性的治疗成功率。
局限性、谨慎原因:绝大多数(90.4%)妇女为白种人,这可能导致该模型在非白种人群中的表现欠佳。我们模型的局限性在于尚未能够对其性能和临床影响进行外部验证,以及预测模型的中等准确性(0.67)。
我们开发了一个预测模型,旨在通过为女性提供其完全排出的个体概率来改善EPL药物治疗的咨询并使其个性化。
研究资金/竞争利益:进行本次二次分析所依据的“Triple M试验”由医疗保险公司创新基金会资助(项目编号3080 B15 - 191)。
Clinicaltrials.gov:NCT03212352