Department of Radiation Oncology, Mayo Clinic, Rochester, MN, USA.
Department of Biomedical Statistics and Informatics, Mayo Clinic, Rochester, MN, USA.
J Hematol Oncol. 2022 Mar 26;15(1):36. doi: 10.1186/s13045-022-01256-w.
F-18 fluorodeoxyglucose positron emission tomography computed tomography (PET/CT) is used to assess response of non-Hodgkin lymphoma (NHL) to chimeric antigen receptor T cell (CAR-T) therapy. We sought to describe metabolic and volumetric PET prognostic factors at one month post-CAR-T and identify which patients with partial response (PR) or stable disease (SD) are most likely to subsequently achieve complete response (CR), and which will develop progressive disease (PD) and death.
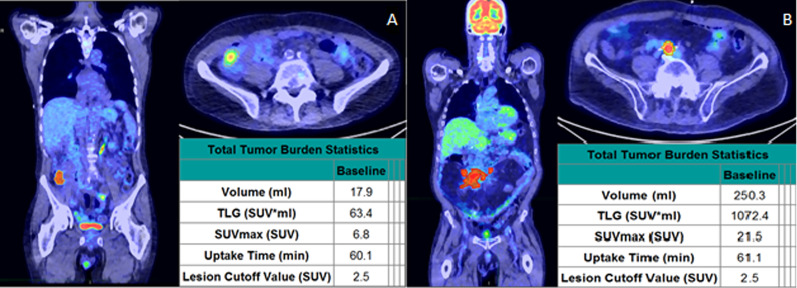
Sixty-nine patients with NHL received axicabtagene ciloleucel CAR-T therapy. One-month post-CAR-T infusion and PET/CT scans were segmented with a fixed absolute SUV maximum (SUVMax) threshold of 2.5 using a semiautomated workflow with manual modification to exclude physiologic uptake as needed. Metabolic tumor volume (MTV), total lesion glycolysis (TLG), SUVMax, and other lesion characteristics were calculated and associated with risk of PD and death.
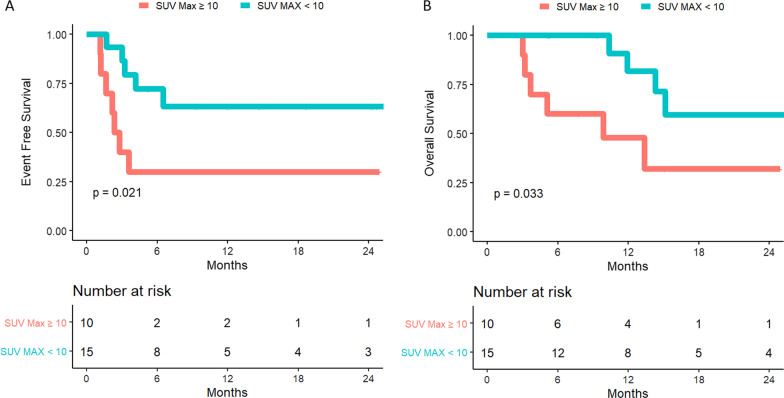
Patients with total MTV > 180 cc, presence of bone or parenchymal disease, SUVMax > 10, single lesion TLG > 245 g, or > 2 total lesions had increased risk of death. Patients with total MTV > 55 cc, total TLG > 250 cc, SUV Max > 10, or > 2 total lesions had increased risk of PD. For the subset of 28 patients with PR/SD, higher SUVMax was associated with increased risk of subsequent PD and death. While 86% of patients who had SUVMax ≥ 10 eventually had PD (HR 3.63, 1.13-11.66, p = 0.03), only 36% of those with SUVMax < 10 had PD.
Higher SUVMax at one month post-CAR-T is associated with higher risk of PD and death. SUVMax ≥ 10 may be useful in guiding early salvage treatment decisions in patients with SD/PR at one month.
F-18 氟代脱氧葡萄糖正电子发射断层扫描计算机断层扫描(PET/CT)用于评估嵌合抗原受体 T 细胞(CAR-T)治疗非霍奇金淋巴瘤(NHL)的反应。我们旨在描述 CAR-T 后一个月的代谢和容积 PET 预后因素,并确定哪些部分缓解(PR)或疾病稳定(SD)的患者最有可能随后获得完全缓解(CR),哪些患者将发展为进展性疾病(PD)和死亡。
69 例 NHL 患者接受 axicabtagene ciloleucel CAR-T 治疗。在 CAR-T 输注后一个月进行 PET/CT 扫描,并使用半自动工作流程,通过手动修改来排除生理性摄取,以固定的绝对 SUV 最大值(SUVMax)阈值 2.5 对其进行分段。计算代谢肿瘤体积(MTV)、总病变糖酵解(TLG)、SUVMax 和其他病变特征,并将其与 PD 和死亡的风险相关联。
总 MTV>180 cc、存在骨或实质疾病、SUVMax>10、单个病变 TLG>245 g 或>2 个总病变的患者死亡风险增加。总 MTV>55 cc、总 TLG>250 cc、SUVMax>10 或>2 个总病变的患者 PD 风险增加。对于 28 例 PR/SD 患者亚组,SUVMax 较高与随后 PD 和死亡的风险增加相关。虽然 SUVMax≥10 的患者中有 86%最终发生 PD(HR 3.63,1.13-11.66,p=0.03),但 SUVMax<10 的患者中只有 36%发生 PD。
CAR-T 后一个月 SUVMax 较高与 PD 和死亡的风险增加相关。SUVMax≥10 可能有助于指导在 CAR-T 后一个月 SD/PR 患者中早期挽救治疗决策。