Camon Ana M, Alonso Rodrigo, Muñoz Francisco J, Cardozo Celia, Bernal-Maurandi Javier, Albiach Laia, Agüero Daiana, Marcos M Angeles, Ambrosioni Juan, Bodro Marta, Chumbita Mariana, De la Mora Lorena, Garcia-Pouton Nicole, Dueñas Gerard, Hernandez-Meneses Marta, Inciarte Alexy, Cuesta Genoveva, Meira Fernanda, Morata Laura, Puerta-Alcalde Pedro, Rico Verónica, Herrera Sabina, Tuset Montse, Castro Pedro, Prieto-González Sergio, Almuedo Alex, Muñoz José, Mensa Josep, Sanjuan Gemma, Nicolas J M, Del Rio Ana, Vila Jordi, García Felipe, Martínez José Antonio, Garcia-Vidal Carolina, Soriano Alex
Department of Infectious Diseases, Hospital Clinic of Barcelona-IDIBAPS, University of Barcelona, C/ Villarroel 170, 08036, Barcelona, Spain.
Department of Microbiology, Hospital Clinic of Barcelona, Barcelona, Spain.
Sci Rep. 2022 Mar 28;12(1):5250. doi: 10.1038/s41598-022-08882-x.
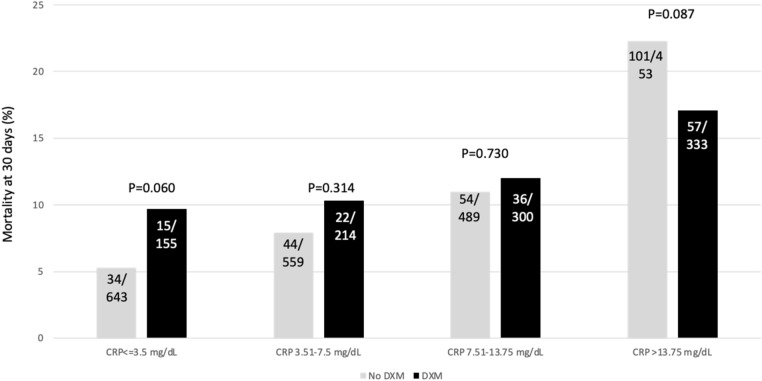
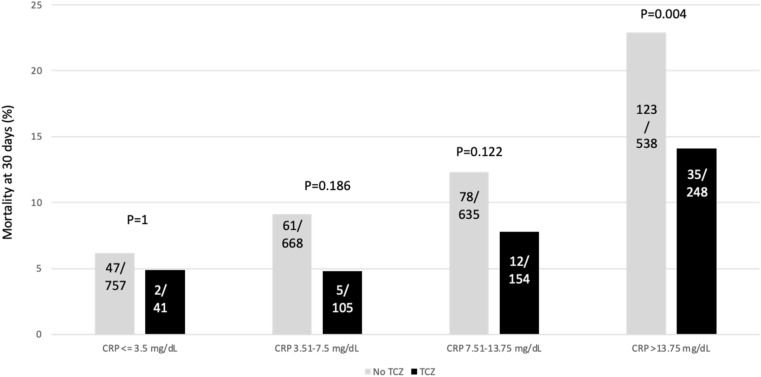
Dexamethasone and tocilizumab have been associated with reduction in mortality, however, the beneficial effect is not for all patients and the impact on viral replication is not well defined. We hypostatized that C-reactive protein (CRP) could help in the identification of patients requiring anti-inflammatory therapy. Patients admitted for > 48 h in our hospital for a confirmed or suspected infection by SARS-CoV-2 from February 2020 to February 2021 were retrospectively evaluated. The primary outcome was mortality at 30 days. Demographics and the most relevant variables related with the outcome were included. CRP was stratified by percentiles. Univariate and multivariate analysis were performed. A total of 3218 patients were included with a median (IQR) age of 66 (74-78) years and 58.9% were males. The rate of intensive care unit admission was 24.4% and the 30-day mortality rate was 11.8%. Within the first 5 days from admission, 1018 (31.7%) patients received dexamethasone and 549 tocilizumab (17.1%). The crude analysis showed a mortality reduction in patients receiving dexamethasone when CRP was > 13.75 mg/dL and > 3.5 mg/dL for those receiving tocilizumab. Multivariate analysis identified the interaction of CRP > 13.75 mg/dL with dexamethasone (OR 0.57; CI 95% 0.37-0.89, P = 0014) and CRP > 3.5 mg/dL with tocilizumab (0.65; CI95%:0.44-0.95, P = 0.029) as independent predictors of mortality. Our results suggest that dexamethasone and tocilizumab are associated with a reduction in mortality when prescribed to patients with a certain inflammatory activity assessed by C-reactive protein.
地塞米松和托珠单抗已被证实与死亡率降低有关,然而,这种有益效果并非对所有患者都适用,且其对病毒复制的影响尚不明确。我们推测C反应蛋白(CRP)有助于识别需要抗炎治疗的患者。对2020年2月至2021年2月期间因确诊或疑似感染新型冠状病毒而在我院住院超过48小时的患者进行了回顾性评估。主要结局是30天死亡率。纳入了人口统计学数据以及与结局最相关的变量。CRP按百分位数分层。进行了单因素和多因素分析。共纳入3218例患者,中位(四分位间距)年龄为66(74 - 78)岁,男性占58.9%。重症监护病房收治率为24.4%,30天死亡率为11.8%。入院后的前5天内,1018例(31.7%)患者接受了地塞米松治疗,549例(17.1%)患者接受了托珠单抗治疗。粗分析显示,CRP > 13.75mg/dL时接受地塞米松治疗的患者死亡率降低,接受托珠单抗治疗的患者CRP > 3.5mg/dL时死亡率降低。多因素分析确定CRP > 13.75mg/dL与地塞米松的相互作用(比值比0.57;95%置信区间0.37 - 0.89,P = 0.014)以及CRP > 3.5mg/dL与托珠单抗的相互作用(0.65;95%置信区间:0.44 - 0.95,P = 0.029)是死亡率的独立预测因素。我们的结果表明,当给通过C反应蛋白评估具有一定炎症活性的患者使用地塞米松和托珠单抗时可降低死亡率。