Department of Intensive Care Medicine, Radboud University Medical Center, Postbus 9101, 6500 HB, Nijmegen, The Netherlands.
Radboud Center for Infectious Diseases, Radboud University Medical Center, 6500 HB, Nijmegen, The Netherlands.
Crit Care. 2021 Aug 5;25(1):281. doi: 10.1186/s13054-021-03717-z.
Procalcitonin (PCT) and C-reactive protein (CRP) were previously shown to have value for the detection of secondary infections in critically ill COVID-19 patients. However, since the introduction of immunomodulatory therapy, the value of these biomarkers is unclear. We investigated PCT and CRP kinetics in critically ill COVID-19 patients treated with dexamethasone with or without tocilizumab, and assessed the value of these biomarkers to detect secondary bacterial infections.
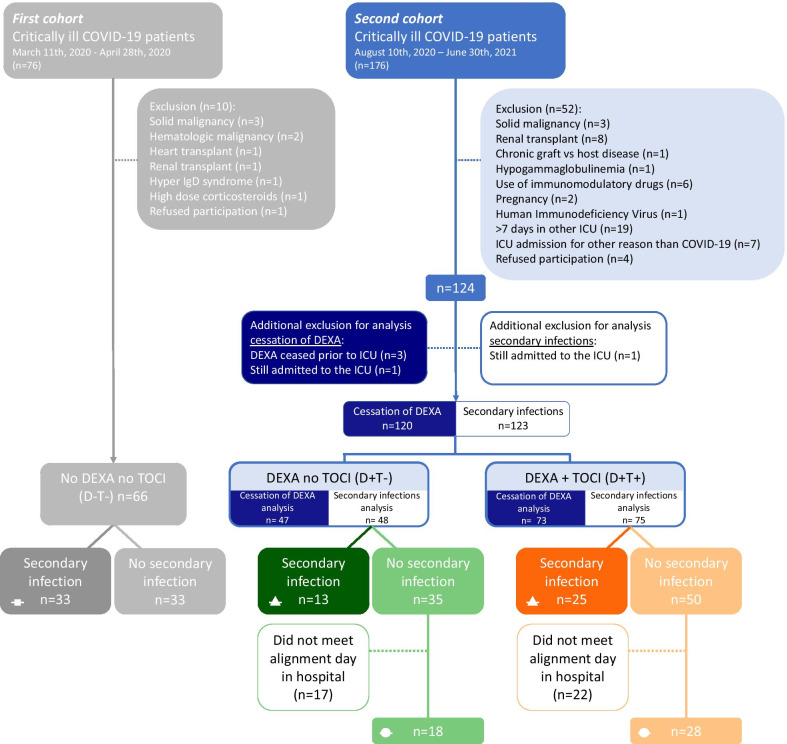
In this prospective study, 190 critically ill COVID-19 patients were divided into three treatment groups: no dexamethasone, no tocilizumab (D-T-), dexamethasone, no tocilizumab (D+T-), and dexamethasone and tocilizumab (D+T+). Serial data of PCT and CRP were aligned on the last day of dexamethasone treatment, and kinetics of these biomarkers were analyzed between 6 days prior to cessation of dexamethasone and 10 days afterwards. Furthermore, the D+T- and D+T+ groups were subdivided into secondary infection and no-secondary infection groups to analyze differences in PCT and CRP kinetics and calculate detection accuracy of these biomarkers for the occurrence of a secondary infection.
Following cessation of dexamethasone, there was a rebound in PCT and CRP levels, most pronounced in the D+T- group. Upon occurrence of a secondary infection, no significant increase in PCT and CRP levels was observed in the D+T- group (p = 0.052 and p = 0.08, respectively). Although PCT levels increased significantly in patients of the D+T+ group who developed a secondary infection (p = 0.0003), this rise was only apparent from day 2 post-infection onwards. CRP levels remained suppressed in the D+T+ group. Receiver operating curve analysis of PCT and CRP levels yielded area under the curves of 0.52 and 0.55, respectively, which are both markedly lower than those found in the group of COVID-19 patients not treated with immunomodulatory drugs (0.80 and 0.76, respectively, with p values for differences between groups of 0.001 and 0.02, respectively).
Cessation of dexamethasone in critically ill COVID-19 patients results in a rebound increase in PCT and CRP levels unrelated to the occurrence of secondary bacterial infections. Furthermore, immunomodulatory treatment with dexamethasone and tocilizumab considerably reduces the value of PCT and CRP for detection of secondary infections in COVID-19 patients.
降钙素原(PCT)和 C 反应蛋白(CRP)以前被证明对检测危重症 COVID-19 患者的继发感染有价值。然而,自从免疫调节治疗引入以来,这些生物标志物的价值尚不清楚。我们研究了接受地塞米松治疗的危重症 COVID-19 患者的 PCT 和 CRP 动力学,并用这些生物标志物来检测继发细菌感染。
在这项前瞻性研究中,190 例危重症 COVID-19 患者分为三组:不使用地塞米松,不使用托珠单抗(D-T-);使用地塞米松,不使用托珠单抗(D+T-);使用地塞米松和托珠单抗(D+T+)。将 PCT 和 CRP 的连续数据与地塞米松治疗的最后一天对齐,并分析在停止地塞米松前 6 天至后 10 天之间这些生物标志物的动力学。此外,将 D+T-和 D+T+组分为继发感染和无继发感染组,以分析 PCT 和 CRP 动力学的差异,并计算这些生物标志物对继发感染发生的检测准确性。
停止地塞米松后,PCT 和 CRP 水平反弹,D+T-组最为明显。发生继发感染时,D+T-组 PCT 和 CRP 水平无明显升高(p=0.052 和 p=0.08)。尽管继发感染的 D+T+组患者的 PCT 水平显著升高(p=0.0003),但这种升高仅在感染后第 2 天才出现。D+T+组的 CRP 水平仍受抑制。PCT 和 CRP 水平的受试者工作特征曲线分析得出的曲线下面积分别为 0.52 和 0.55,均明显低于未接受免疫调节药物治疗的 COVID-19 患者组(分别为 0.80 和 0.76,两组间差异的 p 值均为 0.001 和 0.02)。
停止危重症 COVID-19 患者的地塞米松治疗会导致 PCT 和 CRP 水平反弹,与继发细菌感染无关。此外,地塞米松和托珠单抗的免疫调节治疗大大降低了 PCT 和 CRP 对 COVID-19 患者继发感染的检测价值。