Yin Mengchen, Ding Xing, Zhu Yuefeng, Lin Rui, Sun Yueli, Xiao Yu, Wang Tao, Yan Yinjie, Ma Junming, Mo Wen
Shanghai University of Traditional Chinese Medicine, Shanghai, China.
74754Long hua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, China.
Global Spine J. 2022 Oct;12(8):1956-1967. doi: 10.1177/21925682221084969. Epub 2022 Mar 29.
This is a meta-analysis and systematic review of the available literature.
In the case of severe foraminal stenosis, conducting uncinate process resection (UPR) during ACDF could achieve complete nerve root decompression and significant relief of neurological symptoms for CR. However, there is some controversy regarding its necessity and safety. This study aims to compare the safety and efficacy of ACDF with UPR and ACDF.
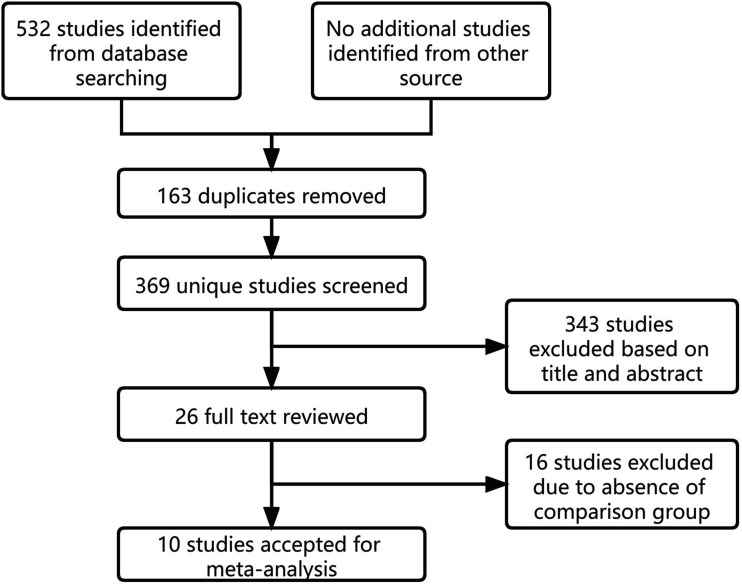
The following electronic databases were searched: Medline, PubMed, Embase, the Cochrane Central Register of Controlled Trials, Evidence Based Medicine Reviews, VIP, and CNKI. And the following data items were considered: baseline demographics, efficacy evaluation indicators, radiographic outcome, and surgical details.
10 studies were finally identified, including 746 patients who underwent ACDF with UPR compared to 729 patients who underwent ACDF. The group of ACDF with UPR had statistically longer intraoperative time (95% CI: 4.83, 19.77, = .001) and more intraoperative blood loss (95% CI: 12.23, 17.76, < .001). ACDF with UPR obtained a significantly better improvement of Arm VAS at postoperative first follow-up (95% CI: -1.85, -.14 = .02). There was no significant difference found in improvement of Neck VAS at postoperative latest follow-up (95% CI: -.88, .27, = .30), improvement of Arm VAS at postoperative latest follow-up (95% CI: -.59, -.01, = .05), improvement of NDI (95% CI: -2.34, .33, = .14), JOA (95% CI: -.24, .43, = .56), change of C2-C7 lordosis (95% CI: -.87, 1.33, = .68), C2-C7 SVA (95% CI: -.73, 5.08, = .14), T1 slope (95% CI: -2.25, 1.51, = .70), and fusion rate (95% CI: .83, 1.90 = .29).
ACDF with UPR is an effective and necessary surgical method for CR patients with severe foraminal stenosis.
这是一项对现有文献的荟萃分析和系统评价。
在严重椎间孔狭窄的情况下,在颈椎前路椎间盘切除融合术(ACDF)期间进行钩突切除术(UPR)可实现神经根的完全减压,并显著缓解神经根型颈椎病(CR)患者的神经症状。然而,其必要性和安全性存在一些争议。本研究旨在比较ACDF联合UPR与单纯ACDF的安全性和有效性。
检索了以下电子数据库:Medline、PubMed、Embase、Cochrane对照试验中心注册库、循证医学综述、维普资讯和中国知网。并考虑了以下数据项:基线人口统计学、疗效评估指标、影像学结果和手术细节。
最终确定了10项研究,其中746例患者接受了ACDF联合UPR,729例患者接受了单纯ACDF。ACDF联合UPR组的术中时间在统计学上更长(95%CI:4.83,19.77,P = 0.001),术中失血量更多(95%CI:12.23,17.76,P < 0.001)。ACDF联合UPR在术后首次随访时臂部视觉模拟评分(VAS)的改善明显更好(95%CI:-1.85,-0.14,P = 0.02)。在术后末次随访时颈部VAS的改善(95%CI:-0.88,0.27,P = 0.30)、术后末次随访时臂部VAS的改善(95%CI:-0.59,-0.01,P = 0.05)、日本骨科学会(JOA)评分的改善(95%CI:-0.24,0.43,P = 0.56)、颈椎功能障碍指数(NDI)的改善(95%CI:-2.34,0.33,P = 0.14)、C2-C7前凸的变化(95%CI:-0.87,1.33,P = 0.68)、C2-C7矢状面垂直轴(SVA)的变化(95%CI:-0.73,5.08,P = 0.14)、T1斜率的变化(95%CI:-2.25,1.51,P = 0.70)以及融合率(95%CI:0.83,1.90,P = 0.29)方面均未发现显著差异。
对于患有严重椎间孔狭窄的CR患者,ACDF联合UPR是一种有效且必要的手术方法。