Hermine Olivier, Mariette Xavier, Porcher Raphael, Djossou Felix, Nguyen Yann, Arlet Jean-Benoît, Savale Laurent, Diehl Jean Luc, Georgin-Lavialle Sophie, Cadranel Jacques, Pialoux Gilles, Lacombe Karine, Mekinian Arsène, Gros Hélène, Lescure Xavier, Ghosn Jade, Coupez Elisabeth, Grapin Kevin, Rapp Christophe, Michel Marc, Lecapitaine Anne Lise, Michot Jean Marie, Costedoat-Chalumeau Nathalie, Nguyen Liem Binh Luong, Semerano Luca, Raffi François, Aguillar Claire, Rouzaud Claire, Gottenberg Jacques Eric, Hansmann Yves, Bienvenu Boris, London Jonathan, Fantchou Franklin Samou, Ackermann Felix, Gros Antoine, Morel Alexandre, Gambier Nicolas, Sène Damien, Mégarbane Bruno, Azoulay Elie, Bureau Serge, Dougados Maxime, Emmerich Joseph, Fartoukh Muriel, Guidet Bertrand, Humbert Marc, Mahevas Mathieu, Pène Frédéric, Schlemmer Frédéric, Pourcher-Martinez Valérie, Tibi Annick, Baron Gabriel, Perrodeau Elodie, Baron Stéphanie, Steg Gabriel, Yazdapanah Yazdan, Simon Tabassome, Resche-Rigon Matthieu, Tharaux Pierre-Louis, Ravaud Philippe
Département d'hématologie, Hôpital Necker, Assistance Publique Hôpitaux de Paris, Université de Paris, 149 rue de Sèvres, Paris 75015, France.
Laboratory of physiopathology and treatment of Hematological malignancies, Institut imagine, INSERM U1153, Université de Paris, Paris, France.
EClinicalMedicine. 2022 Mar 25;46:101362. doi: 10.1016/j.eclinm.2022.101362. eCollection 2022 Apr.
In moderate-to-severe COVID-19 pneumonia, dexamethasone (DEX) and tocilizumab (TCZ) reduce the occurrence of death and ventilatory support. We investigated the efficacy and safety of DEX+TCZ in an open randomized clinical trial.
From July 24, 2020, through May 18, 2021, patients with moderate-to-severe COVID-19 pneumonia requiring oxygen (>3 L/min) were randomly assigned to receive DEX (10 mg/d 5 days tapering up to 10 days) alone or combined with TCZ (8 mg/kg IV) at day 1, possibly repeated with a fixed dose of 400 mg i.v. at day 3. The primary outcome was time from randomization to mechanical ventilation support or death up to day 14, analysed on an intent-to-treat basis using a Bayesian approach. ClinicalTrials.gov number, NCT04476979.
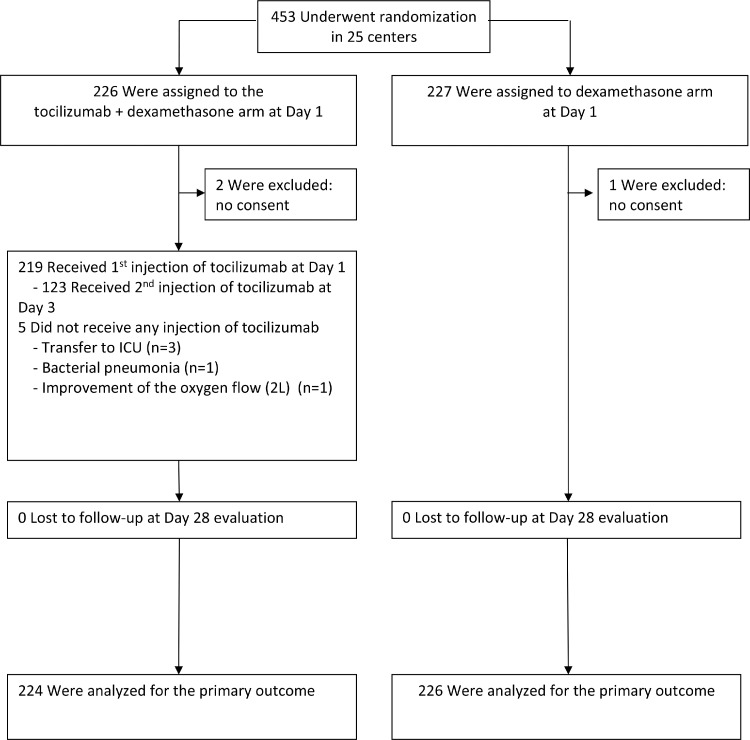
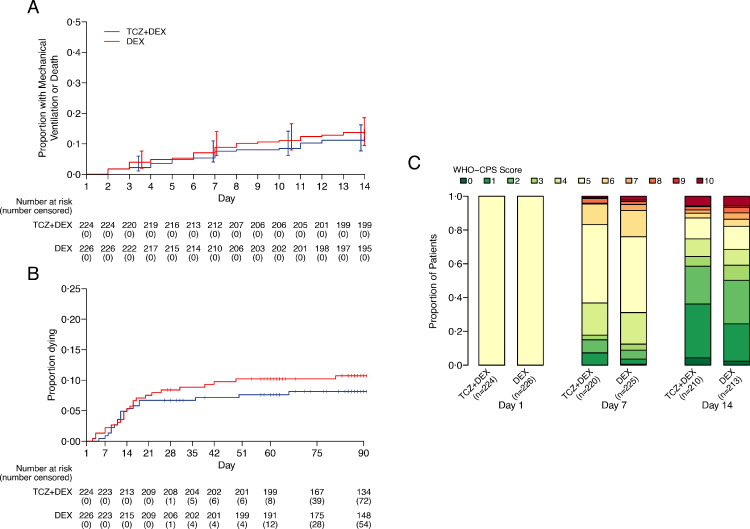
A total of 453 patients were randomized, 3 withdrew consent, 450 were analysed, of whom 226 and 224 patients were assigned to receive DEX or TCZ+DEX, respectively. At day 14, mechanical ventilation or death occurred in 32/226 (14%) and 27/224 (12%) in the DEX and TCZ+DEX arms, respectively (hazard ratio [HR] 0·85, 90% credible interval [CrI] 0·55 to 1·31). At day 14, the World health Organization (WHO) clinical progression scale (CPS) was significantly improved in the TCZ+DEX arm (OR 0·69, 95% CrI, 0·49 to 0.97). At day 28, the cumulative incidence of oxygen supply independency was 82% in the TCZ+DEX arms and 72% in the DEX arm (HR 1·36, 95% CI 1·11 to 1·67). On day 90, 24 deaths (11%) were observed in the DEX arm and 18 (8%) in the TCZ+DEX arm (HR 0·77, 95% CI 0·42-1·41). Serious adverse events were observed in 25% and 21% in DEX and TCZ+DEX arms, respectively.
Mechanical ventilation need and mortality were not improved with TCZ+DEX compared with DEX alone. The safety of both treatments was similar. However, given the wide confidence intervals for the estimate of effect, definitive interpretation cannot be drawn.
Programme Hospitalier de Recherche Clinique [PHRC COVID-19-20-0151, PHRC COVID-19-20-0029], Fondation de l'Assistance Publique - Hôpitaux de Paris (Alliance Tous Unis Contre le Virus) and from Fédération pour la Recherche Médicale" (FRM). Tocilizumab was provided by Roche.
在中重度新型冠状病毒肺炎(COVID-19肺炎)中,地塞米松(DEX)和托珠单抗(TCZ)可降低死亡和通气支持的发生率。我们在一项开放随机临床试验中研究了DEX+TCZ的疗效和安全性。
从2020年7月24日至2021年5月18日,将需要吸氧(>3L/分钟)的中重度COVID-19肺炎患者随机分配,分别接受DEX单药治疗(10mg/天,共5天,逐渐减量至10天)或在第1天联合TCZ(8mg/kg静脉注射),第3天可能重复静脉注射固定剂量400mg。主要结局是从随机分组至第14天需要机械通气支持或死亡的时间,采用贝叶斯方法在意向性分析基础上进行分析。ClinicalTrials.gov编号,NCT04476979。
共453例患者被随机分组,3例撤回同意书,450例接受分析,其中226例和224例患者分别被分配接受DEX或TCZ+DEX治疗。在第14天,DEX组和TCZ+DEX组分别有32/226例(14%)和27/224例(12%)发生机械通气或死亡(风险比[HR]0.85,90%可信区间[CrI]0.55至1.31)。在第14天,TCZ+DEX组世界卫生组织(WHO)临床进展量表(CPS)显著改善(比值比[OR]0.69,95%CrI,0.49至0.97)。在第28天,TCZ+DEX组氧气供应独立的累积发生率为82%,DEX组为72%(HR1.36,95%CI1.11至1.67)。在第90天,DEX组观察到24例死亡(11%),TCZ+DEX组观察到18例死亡(8%)(HR0.77,95%CI0.42 - 1.41)。DEX组和TCZ+DEX组分别有25%和21%的患者出现严重不良事件。
与单独使用DEX相比,TCZ+DEX并未改善机械通气需求和死亡率。两种治疗的安全性相似。然而,鉴于效应估计的置信区间较宽,无法得出明确的解释。
临床研究医院项目[PHRC COVID - 19 - 20 - 0151,PHRC COVID - 19 - 20 - 0029]、巴黎公立医院基金会(联合抗击病毒联盟)以及医学研究联合会(FRM)。托珠单抗由罗氏公司提供。