Department of Molecular Pathology, Netherlands Cancer Institute, Amsterdam, the Netherlands.
Division of Pathology, University Medical Center Utrecht, Utrecht, the Netherlands.
J Clin Oncol. 2022 Jul 20;40(21):2361-2374. doi: 10.1200/JCO.21.01536. Epub 2022 Mar 30.
Triple-negative breast cancer (TNBC) is considered aggressive, and therefore, virtually all young patients with TNBC receive (neo)adjuvant chemotherapy. Increased stromal tumor-infiltrating lymphocytes (sTILs) have been associated with a favorable prognosis in TNBC. However, whether this association holds for patients who are node-negative (N0), young (< 40 years), and chemotherapy-naïve, and thus can be used for chemotherapy de-escalation strategies, is unknown.
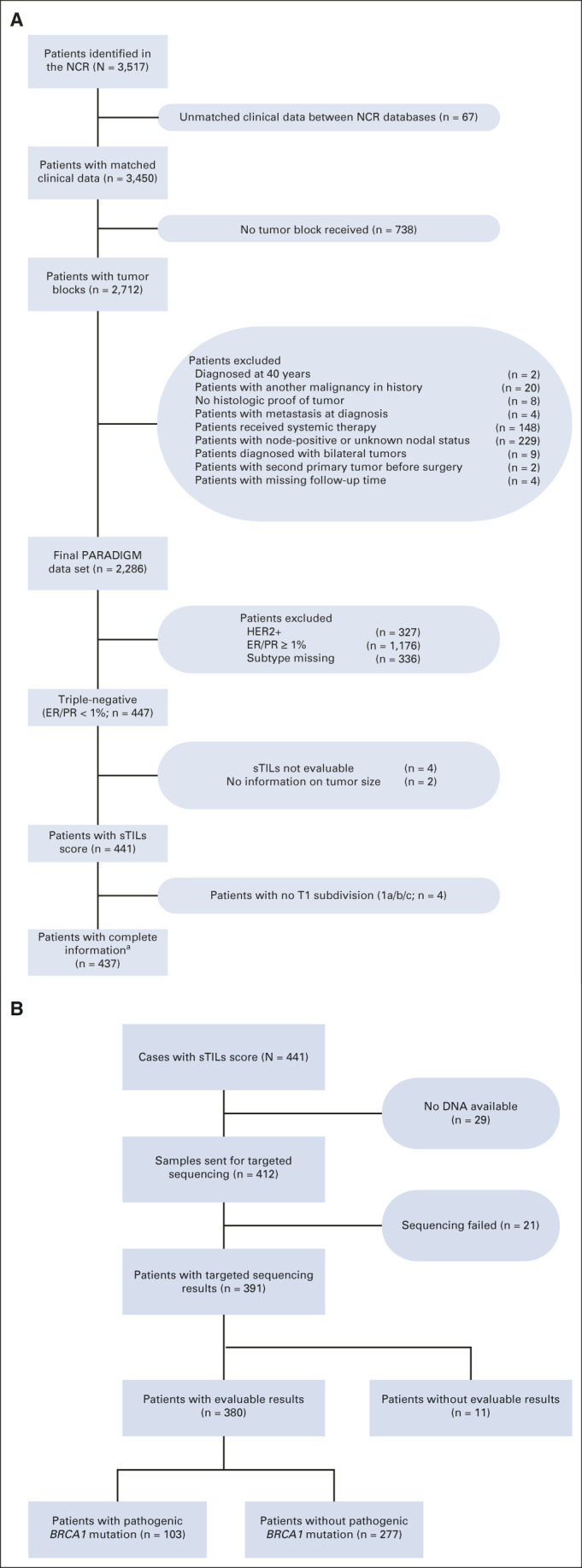
We selected all patients with N0 TNBC diagnosed between 1989 and 2000 from a Dutch population-based registry. Patients were age < 40 years at diagnosis and had not received (neo)adjuvant systemic therapy, as was standard practice at the time. Formalin-fixed paraffin-embedded blocks were retrieved (PALGA: Dutch Pathology Registry), and a pathology review including sTILs was performed. Patients were categorized according to sTILs (< 30%, 30%-75%, and ≥ 75%). Multivariable Cox regression was performed for overall survival, with or without sTILs as a covariate. Cumulative incidence of distant metastasis or death was analyzed in a competing risk model, with second primary tumors as competing risk.
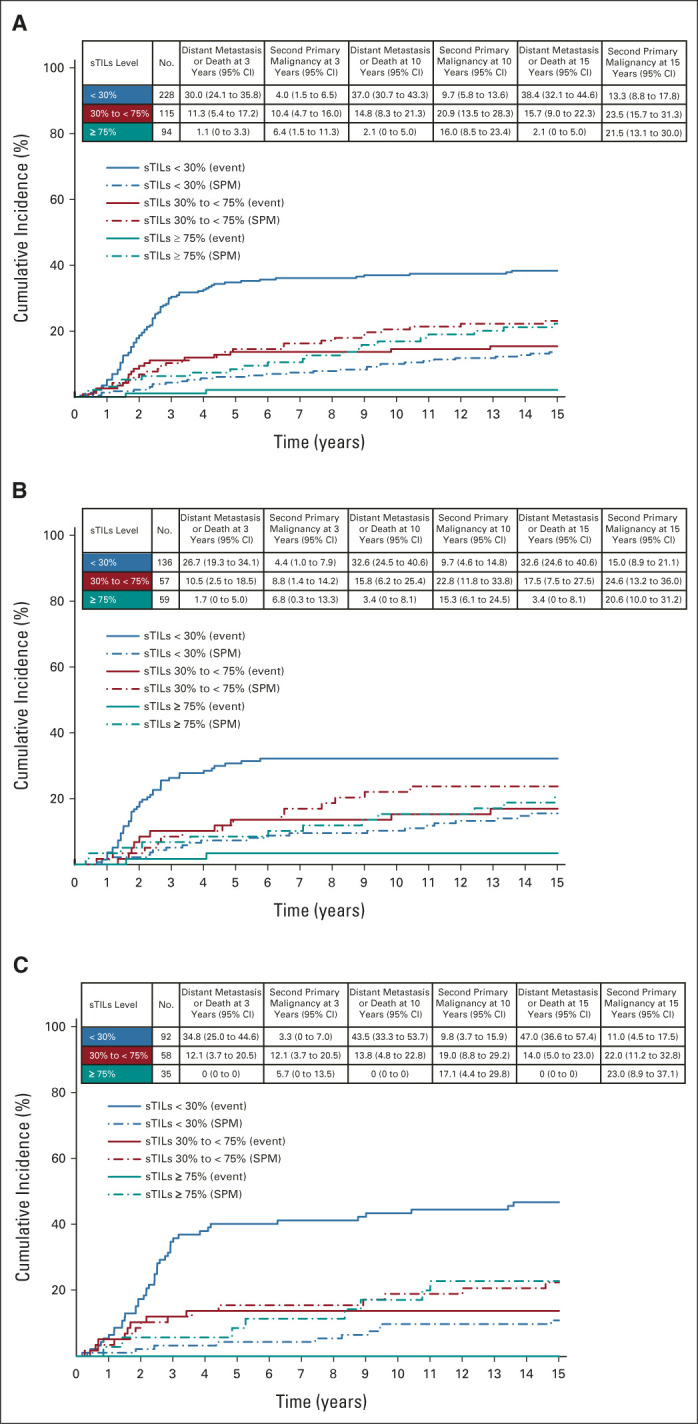
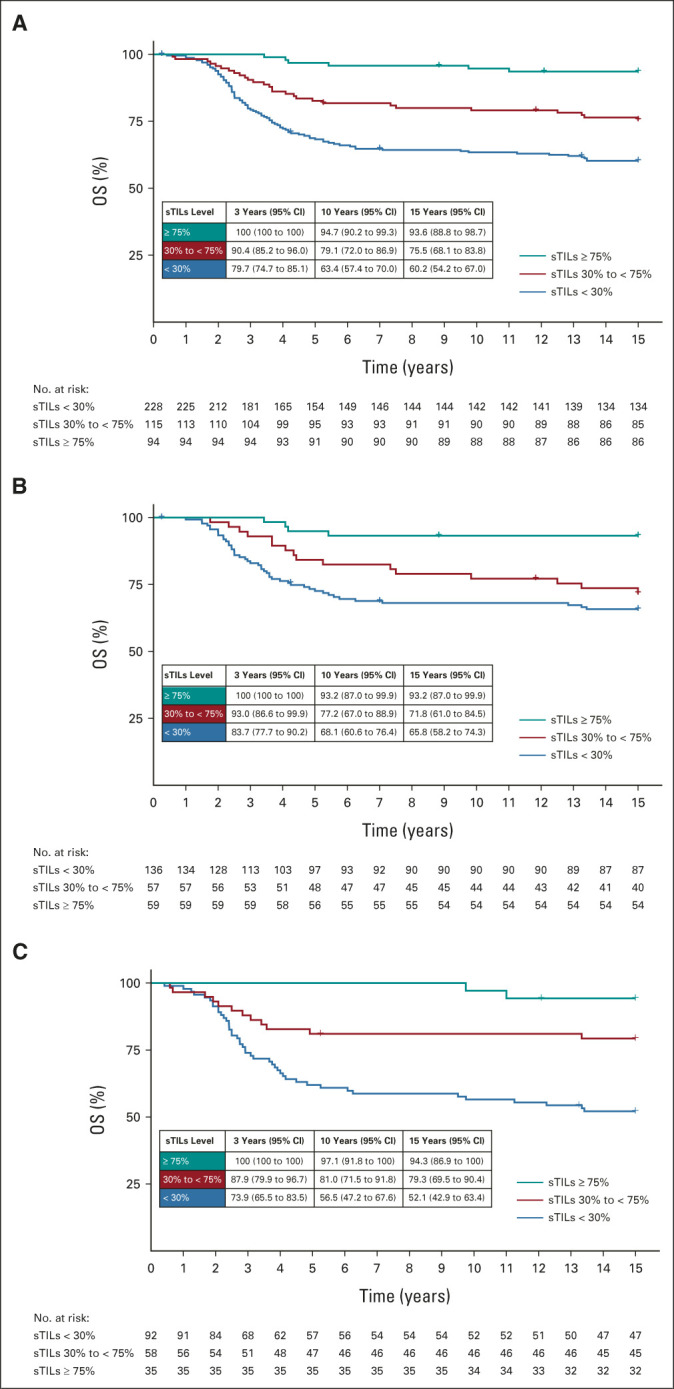
sTILs were scored for 441 patients. High sTILs (≥ 75%; 21%) translated into an excellent prognosis with a 15-year cumulative incidence of a distant metastasis or death of only 2.1% (95% CI, 0 to 5.0), whereas low sTILs (< 30%; 52%) had an unfavorable prognosis with a 15-year cumulative incidence of a distant metastasis or death of 38.4% (32.1 to 44.6). In addition, every 10% increment of sTILs decreased the risk of death by 19% (adjusted hazard ratio: 0.81; 95% CI, 0.76 to 0.87), which are an independent predictor adding prognostic information to standard clinicopathologic variables (χ = 46.7, < .001).
Chemotherapy-naïve, young patients with N0 TNBC with high sTILs (≥ 75%) have an excellent long-term prognosis. Therefore, sTILs should be considered for prospective clinical trials investigating (neo)adjuvant chemotherapy de-escalation strategies.
三阴性乳腺癌(TNBC)被认为具有侵袭性,因此,几乎所有年轻的 TNBC 患者都接受(新)辅助化疗。肿瘤间质浸润淋巴细胞(sTILs)增多与 TNBC 的预后良好相关。然而,对于淋巴结阴性(N0)、年轻(<40 岁)且未经化疗的患者,这种相关性是否存在,以及是否可以用于化疗降阶梯策略,目前尚不清楚。
我们从荷兰人群基础登记处选择了 1989 年至 2000 年间诊断的所有 N0 TNBC 患者。患者在诊断时年龄<40 岁,且未接受(新)辅助系统治疗,这是当时的标准治疗方法。我们检索了福尔马林固定石蜡包埋块(PALGA:荷兰病理登记处),并进行了包括 sTILs 在内的病理复查。根据 sTILs(<30%、30%-75%和≥75%)对患者进行分类。对总生存期进行了多变量 Cox 回归分析,是否包含 sTILs 作为协变量。采用竞争风险模型分析远处转移或死亡的累积发生率,将第二原发肿瘤作为竞争风险。
对 441 例患者进行了 sTILs 评分。高 sTILs(≥75%;21%)预后良好,15 年远处转移或死亡的累积发生率仅为 2.1%(95%CI,0 至 5.0),而低 sTILs(<30%;52%)预后不良,15 年远处转移或死亡的累积发生率为 38.4%(32.1 至 44.6)。此外,sTILs 每增加 10%,死亡风险降低 19%(调整后的危险比:0.81;95%CI,0.76 至 0.87),这是对标准临床病理变量有预后意义的独立预测因素(χ²=46.7,<0.001)。
对于无化疗、年轻、N0 TNBC 且 sTILs 高(≥75%)的患者,其具有极好的长期预后。因此,应考虑将 sTILs 用于前瞻性临床试验,以探讨(新)辅助化疗降阶梯策略。