Department of Obstetrics and Gynecology, Shengjing Hospital of China Medical University, Shenyang, China.
Front Endocrinol (Lausanne). 2022 Mar 8;13:823710. doi: 10.3389/fendo.2022.823710. eCollection 2022.
Studies have shown a high incidence of subclinical hypothyroidism in pregnancy, but the adverse pregnancy outcomes caused by it are not clear. Therefore, we conducted a systematic review and meta-analysis to evaluate the relationship between subclinical hypothyroidism in pregnancy and hypertensive disorders of pregnancy(HDP) to guide clinical practice.
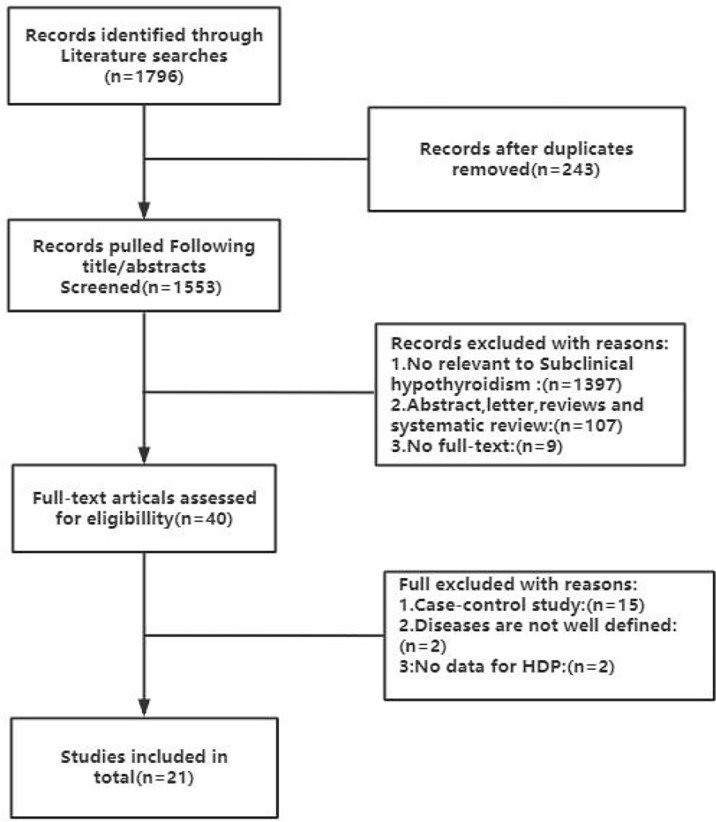
We searched the MEDLINE (PubMed), Cochrane Central, EMBASE, Web of Science, and SCOPUS databases and screened all studies evaluating the relationship between subclinical hypothyroidism in pregnancy and hypertensive disorders of pregnancy. Two researchers independently evaluated the quality of all eligible original studies using the Newcastle-Ottawa Scale (NOS). We also performed a meta-analysis using STATA15.1. Sensitivity analyses were also performed by examining the effects of individual studies as well as using different effect models and detecting any publication bias using the harbord test.
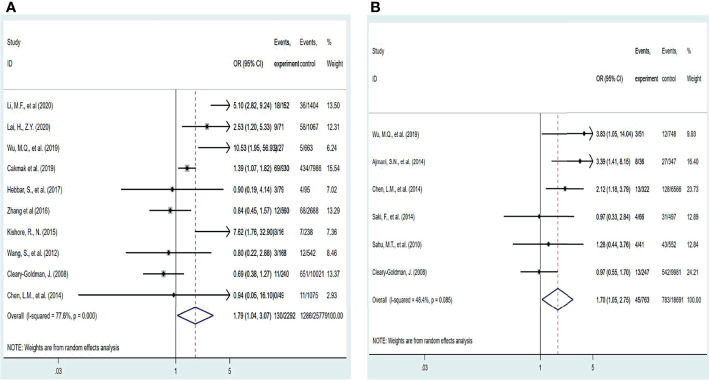
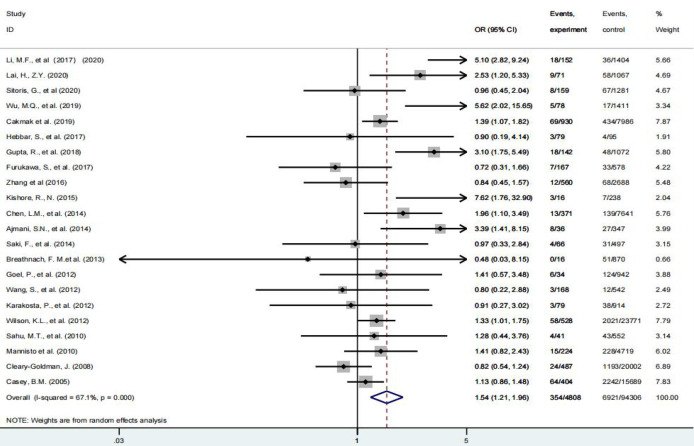
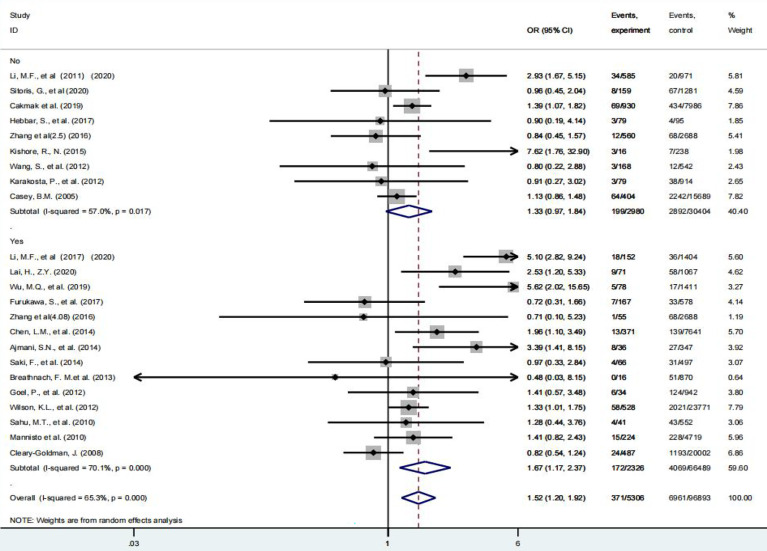
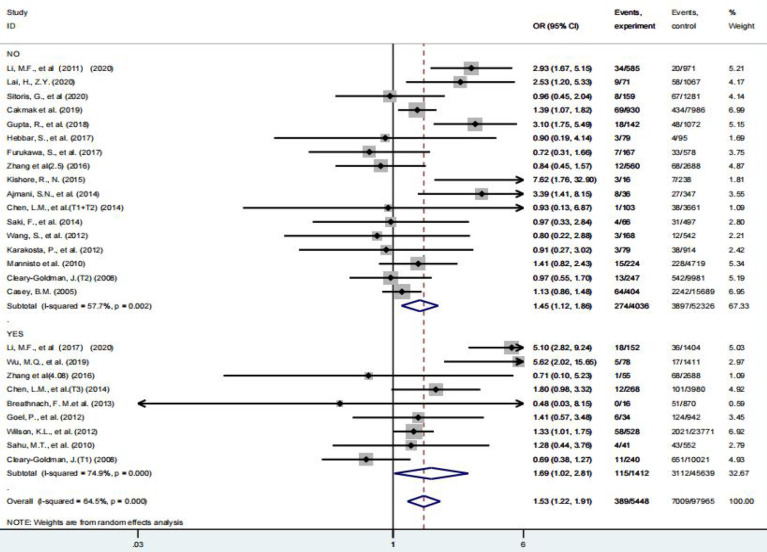
Twenty-two studies were included in the final meta-analysis. Our results indicated that pregnant women with subclinical hypothyroidism had an increased risk of HDP (OR = 1.54(95% CI: 1.21-1.96) I²=67.1%), compared with euthyroidism. Subclinical hypothyroidism in pregnancy was not associated with hypertensive disorders of pregnancy at TSH diagnostic cut-off of less than 3.0 mIU/L (P = 0.077). Curiously, the risk of HDP increases when the TSH diagnostic cut-off value is higher or lower than 4 mIU/L. Although only 9 studies were above the threshold, the risk of developing HDP was still 1.69 times, which was highest in all subgroup analyses. This is consistent with the newly recommended diagnostic cut-off value of 4 mIU/L for TSH by the ATA. Our results consider that the risk of hypertensive disorder complicating pregnancy is increased regardless of the diagnosis of subclinical hypothyroidism at any stage of pregnancy. Unfortunately, there is insufficient evidence to support that patients can benefit from treatment with levothyroxine.
The results of this meta-analysis indicate that subclinical hypothyroidism in pregnancy is associated with an increased risk of developing HDP, and this association exists regardless of the gestational period. However, the available evidence cannot support these patients receiving thyroxine intervention can benefit from it, so routine screening is only recommended for pregnant women with risk factors for hypothyroidism. Further research is needed to validate more scientific and rigorous clinical studies to clarify the relationship between subclinical hypothyroidism and HDP to improve patient prognosis.
https://www.crd.york.ac.uk/prospero/, PROSPERO (CRD42021286405).
研究表明,妊娠亚临床甲状腺功能减退症的发病率很高,但由其引起的不良妊娠结局尚不清楚。因此,我们进行了系统评价和荟萃分析,以评估妊娠亚临床甲状腺功能减退症与妊娠高血压疾病(HDP)之间的关系,从而为临床实践提供指导。
我们检索了 MEDLINE(PubMed)、Cochrane 中心、EMBASE、Web of Science 和 SCOPUS 数据库,并筛选了所有评估妊娠亚临床甲状腺功能减退症与妊娠高血压疾病之间关系的研究。两名研究人员使用纽卡斯尔-渥太华量表(NOS)独立评估所有合格原始研究的质量。我们还使用 STATA15.1 进行了荟萃分析。通过检查个体研究的影响以及使用不同的效应模型和使用哈伯德检验检测任何发表偏倚,也进行了敏感性分析。
最终荟萃分析纳入了 22 项研究。我们的结果表明,与甲状腺功能正常的孕妇相比,妊娠亚临床甲状腺功能减退症患者发生 HDP 的风险增加(OR=1.54(95%CI:1.21-1.96)I²=67.1%)。在 TSH 诊断截断值小于 3.0 mIU/L 时,妊娠亚临床甲状腺功能减退症与妊娠高血压疾病无关(P=0.077)。有趣的是,当 TSH 诊断截断值高于或低于 4 mIU/L 时,HDP 的风险会增加。尽管只有 9 项研究超过了这一阈值,但 HDP 的发病风险仍增加了 1.69 倍,这在所有亚组分析中是最高的。这与 ATA 新推荐的 TSH 诊断截断值 4 mIU/L 一致。我们的结果认为,无论在妊娠的哪个阶段诊断亚临床甲状腺功能减退症,妊娠并发高血压疾病的风险都会增加。遗憾的是,目前没有足够的证据支持这些患者接受左甲状腺素治疗可以从中获益。
这项荟萃分析的结果表明,妊娠亚临床甲状腺功能减退症与 HDP 的发生风险增加有关,这种关联存在于妊娠的任何阶段。然而,现有证据不能支持这些接受甲状腺素干预的患者从中获益,因此仅建议对有甲状腺功能减退症危险因素的孕妇进行常规筛查。需要进一步的研究来验证更科学和严格的临床研究,以阐明亚临床甲状腺功能减退症与 HDP 之间的关系,从而改善患者的预后。
https://www.crd.york.ac.uk/prospero/,PROSPERO(CRD42021286405)。