Department of Radiation Oncology, Ningbo Medical Center Lihuili Hospital, Ningbo University, Ningbo, China.
Department of Surgery, Yuyao Maternity and Child Health Care Hospital, Ningbo, China.
Dis Markers. 2022 Mar 20;2022:5879137. doi: 10.1155/2022/5879137. eCollection 2022.
A phase III randomized multicenter trial (ALTER0303) reported anlotinib to be significantly beneficial to patient survival. An array of inflammatory biomarkers, such as neutrophil lymphocyte ratio (NLR) and platelet lymphocyte ratio (PLR), are associated with the response to treatment in numerous types of cancer. However, we found few studies investigating the predictive value of NLR or PLR in advanced NSCLC treatment with anlotinib. Thus, our objective was to examine the relationship between NLR and PLR and treatment effect, as well as to individuate patient stratification and selection.
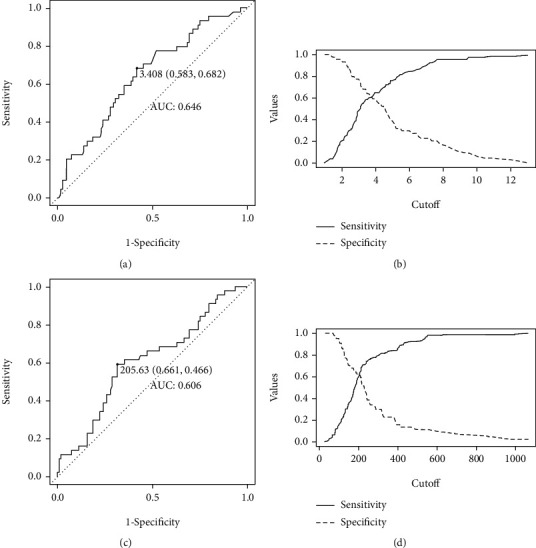
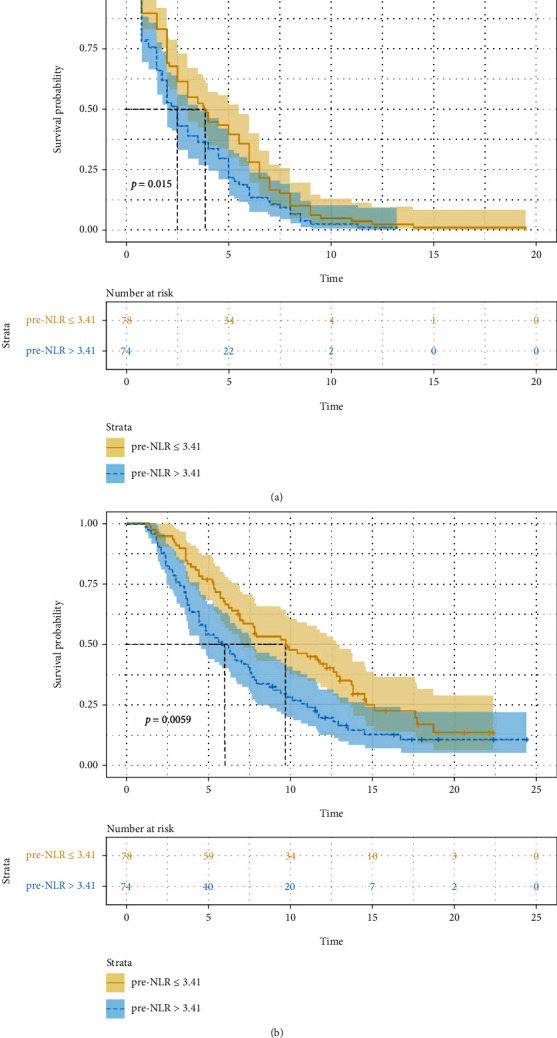
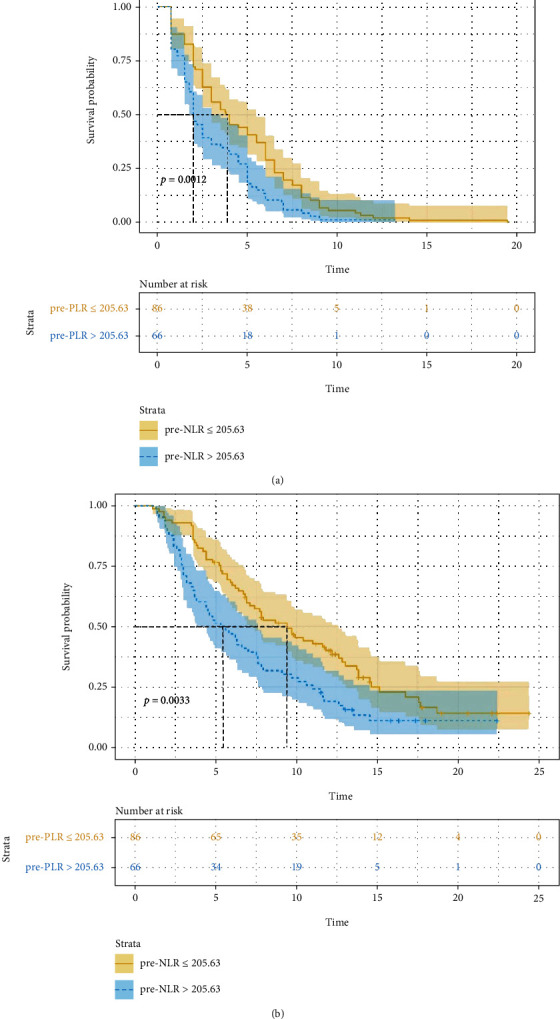
NLR and PLR as well as their variations were calculated in 152 advanced NSCLC patients receiving anlotinib as a third or further-line treatment at Ningbo Medical Center Lihuili Hospital between July 2018 and December 2020. The best cut-off values of NLR and PLR for predicting the treatment response were selected. Survival curves were plotted using the Kaplan-Meier method, while univariable and multivariable Cox regression were used to identify and determine dependent and independent predictors of survival.
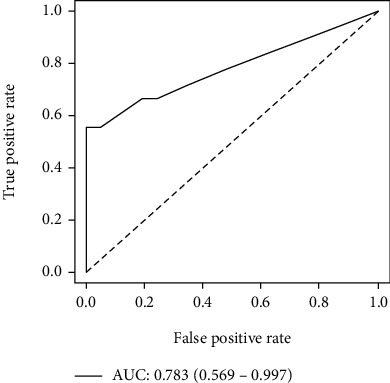
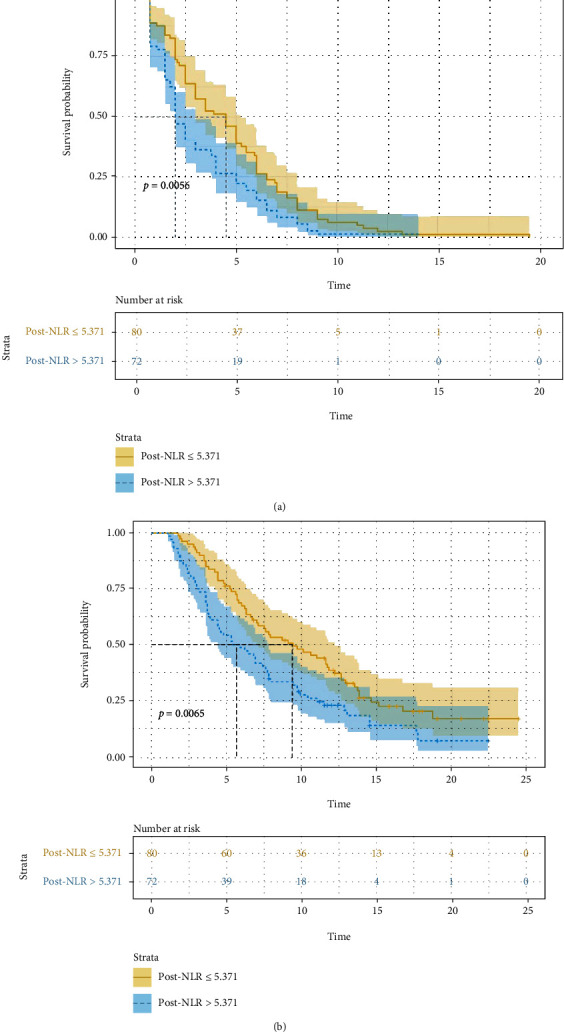
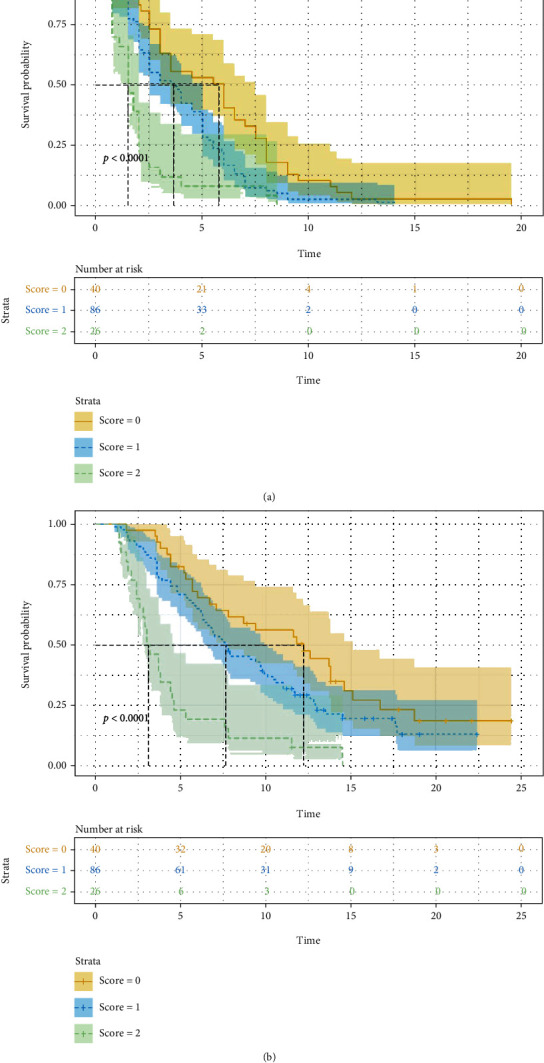
, Low disease control rate (DCR) was related with a high pre-NLR ( = 0.007), high pre-PLR ( = 0.004), and elevated post-NLR ( = 0.010). Multivariate analysis determined high pre-PLR (>205.63) and elevated post-NLR to be independently associated with poor PFS or OS. Patients whose risk score was 2 resulting from the prediction model based on pre-PLR and post-NLR had a 4.52 times higher risk of death compared to patients whose risk score was 0 (HR: 4.516, 95% CI: 2.502-8.152, ≤ 0.001).
Pre-PLR and post-NLR were independent prognostic indicators in patients with advanced NSCLC receiving anlotinib as a third or further-line treatment. Patients whose risk value score was 0 had a higher therapy effectiveness and better survival.
一项 III 期随机多中心试验(ALTER0303)报道安罗替尼显著有益于患者生存。许多类型的癌症中,中性粒细胞与淋巴细胞比值(NLR)和血小板与淋巴细胞比值(PLR)等一系列炎症生物标志物与治疗反应相关。然而,我们发现很少有研究调查 NLR 或 PLR 预测晚期非小细胞肺癌(NSCLC)接受安罗替尼治疗的疗效。因此,我们的目的是研究 NLR 和 PLR 与治疗效果的关系,并确定患者分层和选择。
2018 年 7 月至 2020 年 12 月,在宁波医疗中心李惠利医院,对 152 例接受安罗替尼三线或三线以上治疗的晚期 NSCLC 患者计算 NLR 和 PLR 及其变化。选择 NLR 和 PLR 预测治疗反应的最佳截断值。使用 Kaplan-Meier 法绘制生存曲线,单变量和多变量 Cox 回归用于识别和确定生存的依赖性和独立性预测因素。
低疾病控制率(DCR)与较高的治疗前 NLR(=0.007)、较高的治疗前 PLR(=0.004)和升高的治疗后 NLR(=0.010)相关。多变量分析确定高治疗前 PLR(>205.63)和升高的治疗后 NLR 与较差的无进展生存期(PFS)或总生存期(OS)独立相关。基于治疗前 PLR 和治疗后 NLR 的预测模型,风险评分 2 的患者死亡风险比风险评分 0 的患者高 4.52 倍(HR:4.516,95%CI:2.502-8.152,≤0.001)。
治疗前 PLR 和治疗后 NLR 是接受安罗替尼三线或三线以上治疗的晚期 NSCLC 患者的独立预后指标。风险值评分 0 的患者治疗效果更高,生存更好。