Faehling Martin, Witte Hanno, Sebastian Martin, Ulmer Matthias, Sätzler Rainer, Steinestel Konrad, Brückl Wolfgang M, Evers Georg, Büschenfelde Christian Meyer Zum, Bleckmann Annalen
Department of Cardiology and Pneumology, Hospital Esslingen, Esslingen 73730, Germany.
Abteilung für Hämatologie und Onkologie, Bundeswehrkrankenhaus, Ulm, Germany.
Ther Adv Med Oncol. 2022 Mar 25;14:17588359221085333. doi: 10.1177/17588359221085333. eCollection 2022.
Recent clinical trials demonstrate the feasibility of neoadjuvant immuno(chemo)therapy and report high rates of pathological remission, a surrogate marker for overall survival.
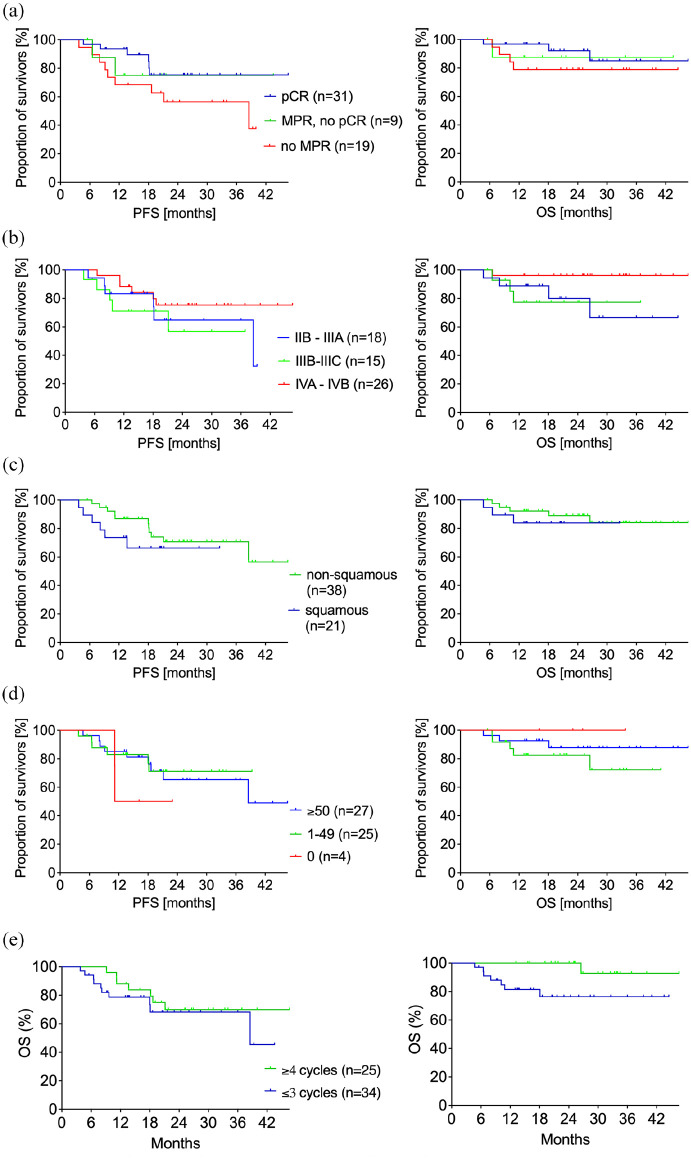
This is a retrospective multicentre real-world analysis of patients with locally resectable NSCLC, including oligometastatic disease, who received neoadjuvant immuno(chemo)therapy and resection. Consolidating immunotherapy was applied following multidisciplinary board recommendation. Primary endpoint was the rate of complete pathological response (pCR, no residual vital tumour cells) or major pathological response (MPR, ⩽ 10% residual vital tumour cells). Secondary endpoints included the radiological response and survival.
Seven centres contributed 59 patients (56% stage IIB-IIIC, 44% in stage IVA-IVB with up to four oligometastatic sites). MPR was found in 68% including 53% with pCR. There were no radiological progressions. Median follow-up was 24.3 months. At 12 and 24 months, progression-free survival was 82.6% and 68.1%, and overall survival was 89.5% and 87.2%, respectively.
To our knowledge, this study encompassed the largest NSCLC real-world cohort treated with neoadjuvant immuno(chemo)therapy to date. In routine clinical practice, resection after neoadjuvant immuno(chemo)therapy is feasible in patients with locally resectable NSCLC, including oligometastatic disease. In line with clinical trials, we found MPR in more than two-thirds of patients. Early data show encouraging survival.
近期临床试验证明了新辅助免疫(化疗)疗法的可行性,并报告了较高的病理缓解率,这是总生存期的替代指标。
这是一项对局部可切除的非小细胞肺癌患者(包括寡转移疾病患者)进行的回顾性多中心真实世界分析,这些患者接受了新辅助免疫(化疗)疗法及手术切除。巩固性免疫治疗根据多学科委员会的建议应用。主要终点是完全病理缓解率(pCR,无残留存活肿瘤细胞)或主要病理缓解率(MPR,残留存活肿瘤细胞≤10%)。次要终点包括影像学缓解和生存率。
七个中心纳入了59例患者(56%为IIB-IIIC期,44%为IVA-IVB期,寡转移部位最多四个)。68%的患者达到MPR,其中53%达到pCR。未出现影像学进展。中位随访时间为24.3个月。在12个月和24个月时,无进展生存率分别为82.6%和68.1%,总生存率分别为89.5%和87.2%。
据我们所知,本研究涵盖了迄今为止接受新辅助免疫(化疗)疗法治疗的最大规模非小细胞肺癌真实世界队列。在常规临床实践中,新辅助免疫(化疗)疗法后进行手术切除对于局部可切除的非小细胞肺癌患者(包括寡转移疾病患者)是可行的。与临床试验一致,我们发现超过三分之二的患者达到MPR。早期数据显示出生存率令人鼓舞。