Pang Naidong, Gao Jia, Zhang Nan, Zhang Binghang, Wang Rui
The First Clinical Medical College, Shanxi Medical University, Taiyuan, Shanxi, China.
Department of Cardiology, First Hospital of Shanxi Medical University, Taiyuan, Shanxi, China.
Cardiol Res Pract. 2022 Mar 20;2022:1124372. doi: 10.1155/2022/1124372. eCollection 2022.
Catheter ablation has become a widely applied intervention for treating symptomatic atrial fibrillation (AF), which can be performed under general anesthesia (GA), deep sedation, or conscious sedation (CS). But the strategy of anesthesia remains controversial.
This systematic review and meta-analysis aims to compare the advantages of GA/deep sedation and CS in AF catheter ablation, including procedural parameters and clinical outcomes.
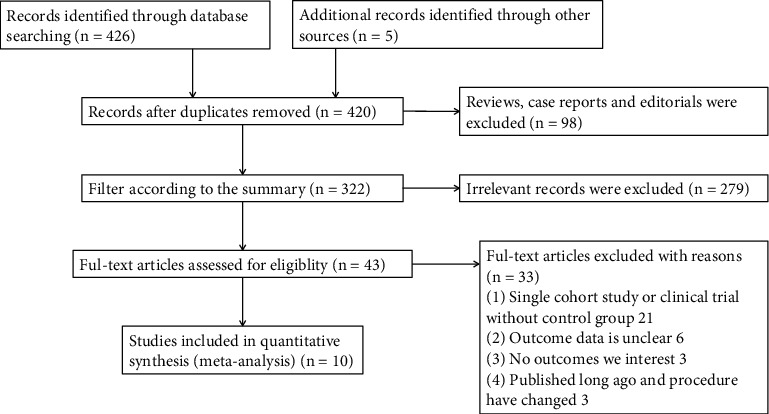
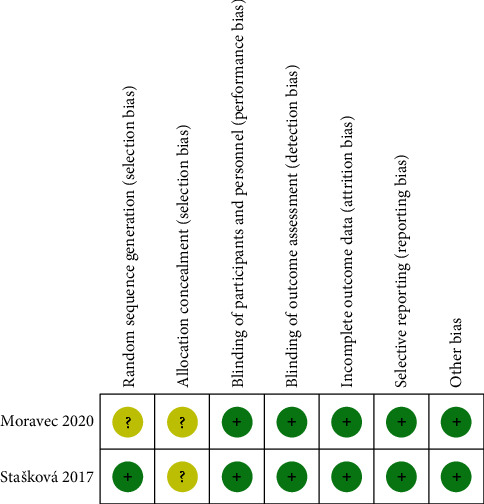
PubMed, Embase, and the Cochrane Library were searched up to November 2021 for randomized controlled trials and observational studies that assessed the outcomes of catheter ablation under GA/deep sedation or CS. Ten studies were included in this meta-analysis after screening with the inclusion and exclusion criteria. Heterogeneity between studies was evaluated by the I index and the Cochran test, respectively; sensitivity analysis including meta-regression was performed if heterogeneity was high. Publication bias was assessed using a funnel plot and Egger' test.
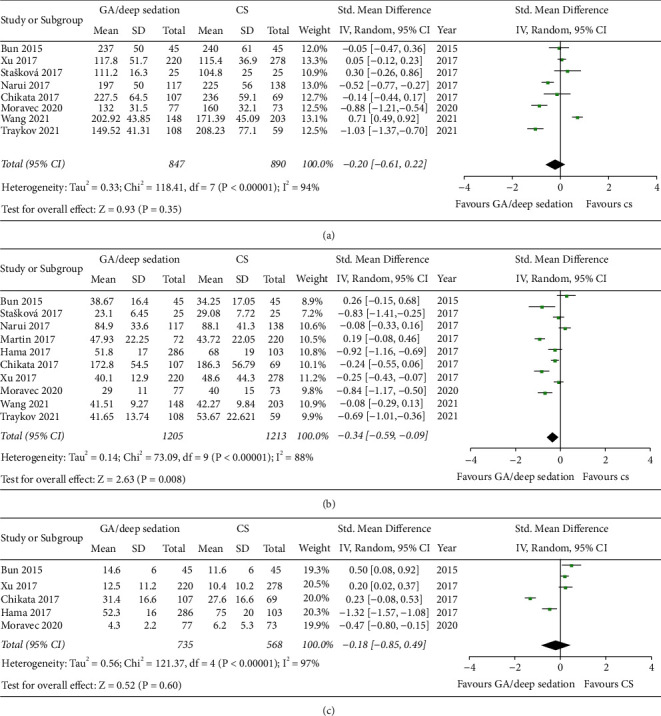
This meta-analysis found GA/deep sedation to be associated with a lower recurrence rate of AF catheter ablation (=0.03). In terms of procedural parameters, there was no significant difference between the two groups for the procedural time (=0.35) and the fluoroscopy time (=0.60), while the ablation time was shorter in the GA/deep sedation group (=0.008). The total complication rate and the incidence of serious adverse events were statistically insignificant between the two groups (=0.07 and =0.94). Meta-regression did not suggest any covariates as an influential factor for procedural parameters and clinical outcomes.
GA/deep sedation may reduce the risk of recurrence after AF ablation without increasing the incidence of complications. GA/deep sedation shortens the ablation duration, although there is no statistical difference in other procedural parameters between GA/deep sedation and CS.
导管消融术已成为治疗症状性心房颤动(AF)广泛应用的干预措施,可在全身麻醉(GA)、深度镇静或清醒镇静(CS)下进行。但麻醉策略仍存在争议。
本系统评价和荟萃分析旨在比较GA/深度镇静与CS在AF导管消融中的优势,包括手术参数和临床结果。
检索截至2021年11月的PubMed、Embase和Cochrane图书馆,查找评估GA/深度镇静或CS下导管消融结果的随机对照试验和观察性研究。经纳入和排除标准筛选后,本荟萃分析纳入了10项研究。分别采用I指数和Cochran检验评估研究间的异质性;如果异质性较高,则进行包括元回归在内的敏感性分析。使用漏斗图和Egger检验评估发表偏倚。
本荟萃分析发现GA/深度镇静与AF导管消融较低的复发率相关(=0.03)。在手术参数方面,两组在手术时间(=0.35)和透视时间(=0.60)上无显著差异,而GA/深度镇静组的消融时间较短(=0.008)。两组的总并发症发生率和严重不良事件发生率在统计学上无显著差异(=0.07和=0.94)。元回归未提示任何协变量是手术参数和临床结果的影响因素。
GA/深度镇静可能降低AF消融术后的复发风险,而不增加并发症发生率。GA/深度镇静缩短了消融持续时间,尽管GA/深度镇静与CS在其他手术参数上无统计学差异。