Safety and Epidemiology, HealthCore Inc., Wilmington, DE.
IBM Watson Health, Littleton.
Clin J Pain. 2022 Jun 1;38(6):396-404. doi: 10.1097/AJP.0000000000001034.
OxyContin was reformulated with a polyethylene oxide matrix in August 2010 to reduce the potential for intravenous abuse and for abuse by insufflation. The objective of this study was to evaluate the impact of OxyContin's reformulation on overdose (OD) risk for individuals dispensed OxyContin in comparison to those dispensed other opioids under regular care.
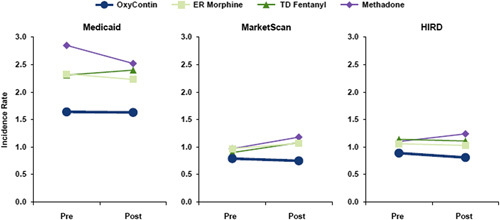
Three national insurance databases with National Death Index linkage identified OD in individuals with any dispensing of OxyContin or a primary comparator opioid (extended release morphine, transdermal fentanyl, or methadone) between July 2008 through September 2015. A difference-in-differences design was used to compare the pre-post reformulation changes in OD rates for OxyContin versus comparators.
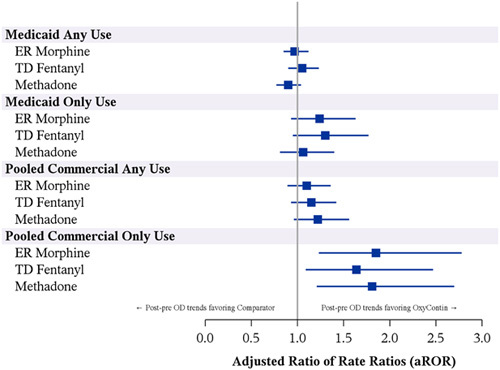
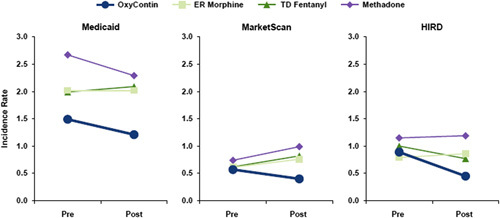
A total of 297,836 individuals were dispensed OxyContin and 659,673 individuals were dispensed a primary comparator across the 3 databases. Overall, there was little or no difference in the temporal change in OD incidence in comparators versus OxyContin (Medicaid: adjusted ratio-of-rate-ratios (aRoRs) ranging from 0.90 to 1.05; MarketScan/HIRD: aRoR ranging from 1.10 to 1.22). However, restriction to person-time without concomitant opioid use revealed a modestly greater reduction in OD incidence over time during OxyContin use, as the aRoRs comparing the primary comparators to OxyContin ranged from 1.06 to 1.30 in Medicaid and from 1.64 to 1.85 in MarketScan/HIRD.
This study did not detect an overall effect of the OxyContin reformulation on OD in insured patients under regular medical care. There is a suggestion of a modestly reduced OxyContin-associated OD risk following the reformulation but only in commercially insured individuals receiving single-opioid regimens.
奥施康定于 2010 年 8 月进行了配方改革,加入了聚乙烯氧化物基质,以减少静脉注射滥用和通过吹管吸食的可能性。本研究的目的是评估奥施康定配方改革对接受奥施康定处方治疗的个体与接受常规护理下其他阿片类药物处方治疗的个体的过量用药(OD)风险的影响。
通过三个具有国家死亡索引链接的国家保险数据库,在 2008 年 7 月至 2015 年 9 月期间,确定了任何奥施康定或主要对照阿片类药物(缓释吗啡、透皮芬太尼或美沙酮)处方的个体的 OD。采用差异中的差异设计比较奥施康定与对照药物在配方改革前后 OD 发生率的变化。
在这三个数据库中,共有 297836 名患者接受了奥施康定处方治疗,659673 名患者接受了主要对照药物处方治疗。总体而言,在对照药物与奥施康定相比,OD 发生率的时间变化几乎没有差异(医疗补助:调整后的比率比(aRoR)范围从 0.90 到 1.05;市场扫描/ HIRD:aRoR 范围从 1.10 到 1.22)。然而,限制无同时使用阿片类药物的个体时间发现,在奥施康定使用期间,OD 发生率随时间适度降低,因为 Medicaid 中主要对照药物与奥施康定相比的 aRoR 范围从 1.06 到 1.30,而 MarketScan/HIRD 中的 aRoR 范围从 1.64 到 1.85。
本研究未发现奥施康定配方改革对常规医疗护理下保险患者的 OD 有总体影响。在配方改革后,奥施康定相关 OD 风险略有降低,但仅在接受单一阿片类药物方案的商业保险个体中。