Clinical Division and Laboratory of Intensive Care Medicine, Department of Cellular and Molecular Medicine, KU Leuven University, B-3000 Leuven, Belgium.
J Clin Endocrinol Metab. 2022 Jun 16;107(7):2057-2064. doi: 10.1210/clinem/dgac201.
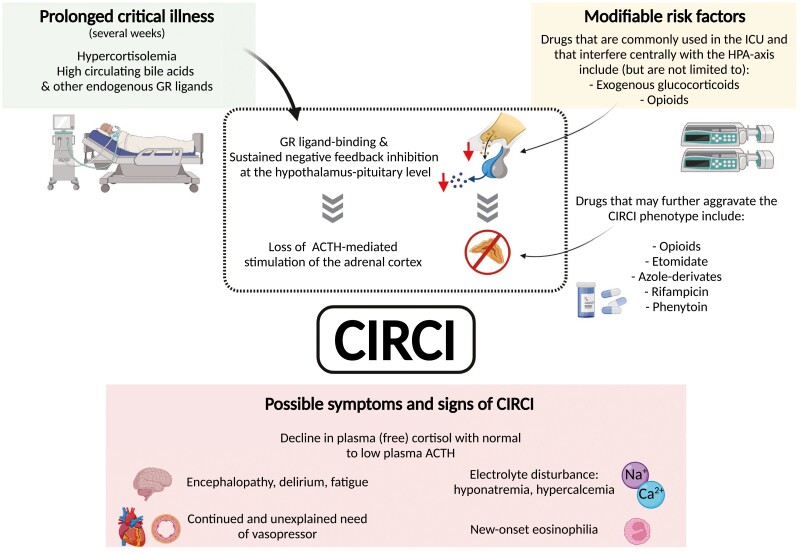
Critical illnesses are hallmarked by increased systemic cortisol availability, a vital part of the stress response. Acute stress may trigger a life-threatening adrenal crisis when a disease of the hypothalamic-pituitary-adrenal (HPA) axis is present and not adequately treated with stress doses of hydrocortisone. Stress doses of hydrocortisone are also used to reduce high vasopressor need in patients suffering from septic shock, in the absence of adrenal insufficiency. Research performed over the last 10 years focusing on the HPA axis during critical illness has led to the insight that neither of these conditions can be labeled "critical illness-induced corticosteroid insufficiency" or CIRCI. Instead, these data suggested using the term CIRCI for a condition that may develop in prolonged critically ill patients. Indeed, when patients remain dependent on vital organ support for weeks, they are at risk of acquiring central adrenal insufficiency. The sustained increase in systemic glucocorticoid availability, mainly brought about by suppressed circulating cortisol-binding proteins and suppressed hepatic/renal cortisol metabolism, exerts negative feedback inhibition at the hypothalamus/pituitary, while high levels of other glucocorticoid receptor ligands, such as bile acids, and drugs, such as opioids, may further suppress adrenocorticotropic hormone (ACTH) secretion. The adrenal cortex, depleted from ACTH-mediated trophic signaling for weeks, may become structurally and functionally impaired, resulting in insufficient cortisol production. Such a central HPA axis suppression may be maladaptive by contributing to lingering vasopressor need and encephalopathy, hence preventing recovery. Here, we review this concept of CIRCI and we advise on how to recognize and treat this poorly understood condition.
危重病的特点是全身性皮质醇可用性增加,这是应激反应的重要组成部分。急性应激可能会引发危及生命的肾上腺危象,如果存在下丘脑-垂体-肾上腺(HPA)轴疾病并且未用皮质醇应激剂量充分治疗,则会发生这种情况。在没有肾上腺功能不全的情况下,皮质醇应激剂量也用于减少患有败血症性休克的患者的高升压剂需求。在过去的 10 年中,针对危重病期间 HPA 轴的研究使人们认识到,这两种情况都不能被标记为“危重病诱导的皮质激素不足”或 CIRCI。相反,这些数据表明,对于可能在长时间危重病患者中发展的情况,可以使用 CIRCI 一词。实际上,当患者依赖重要器官支持数周时,他们有发生中心肾上腺功能不全的风险。系统糖皮质激素可用性的持续增加,主要是由于循环皮质醇结合蛋白的抑制和肝/肾皮质醇代谢的抑制所致,在下丘脑/垂体处产生负反馈抑制,而其他糖皮质激素受体配体(如胆汁酸)和药物(如阿片类药物)的高水平可能进一步抑制促肾上腺皮质激素(ACTH)的分泌。肾上腺皮质由于 ACTH 介导的营养信号传递而持续数周被耗尽,可能会在结构和功能上受损,导致皮质醇产生不足。这种中枢 HPA 轴抑制可能是适应不良的,因为它会导致持续的升压剂需求和脑病,从而阻碍恢复。在这里,我们回顾了 CIRCI 的概念,并就如何识别和治疗这种了解甚少的情况提供了建议。