Clinical Division and Laboratory of Intensive Care Medicine, Department of Cellular and Molecular Medicine, KU Leuven, Herestraat 49, 3000, Leuven, Belgium.
Crit Care. 2021 Feb 16;25(1):65. doi: 10.1186/s13054-021-03475-y.
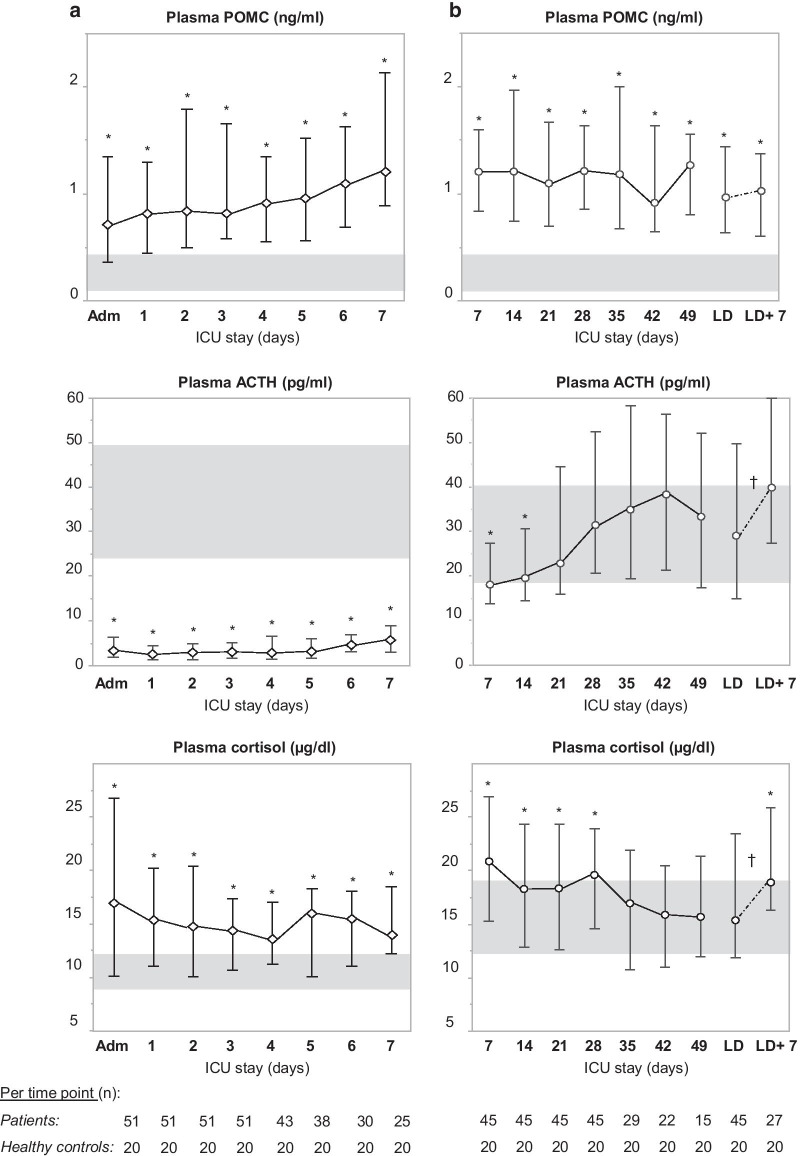
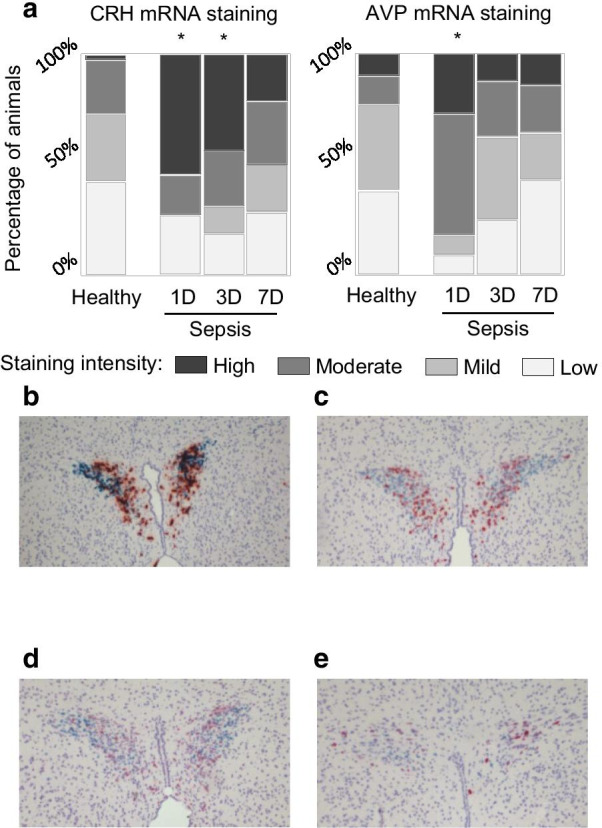
Sepsis is typically hallmarked by high plasma (free) cortisol and suppressed cortisol breakdown, while plasma adrenocorticotropic hormone (ACTH) is not increased, referred to as 'ACTH-cortisol dissociation.' We hypothesized that sepsis acutely activates the hypothalamus to generate, via corticotropin-releasing hormone (CRH) and vasopressin (AVP), ACTH-induced hypercortisolemia. Thereafter, via increased availability of free cortisol, of which breakdown is reduced, feedback inhibition at the pituitary level interferes with normal processing of pro-opiomelanocortin (POMC) into ACTH, explaining the ACTH-cortisol dissociation. We further hypothesized that, in this constellation, POMC leaches into the circulation and can contribute to adrenocortical steroidogenesis.
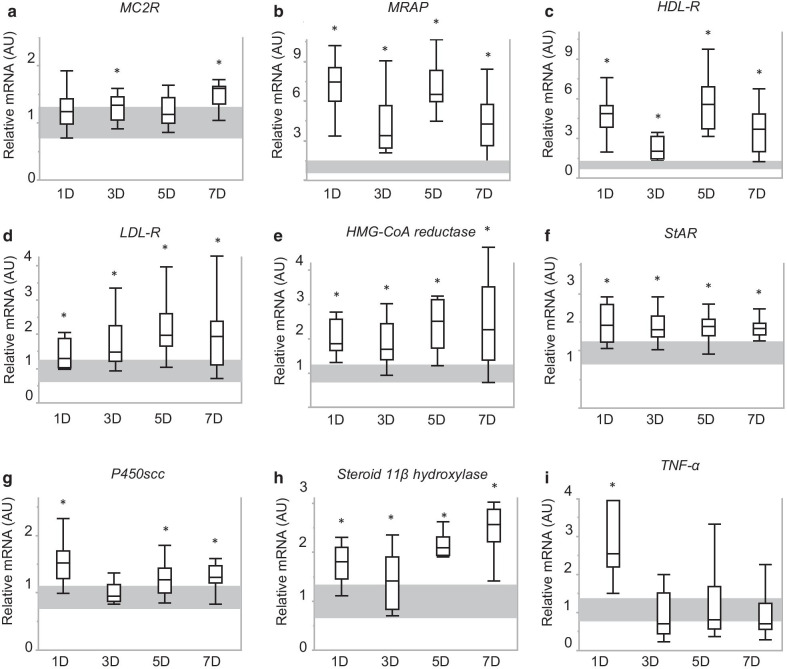
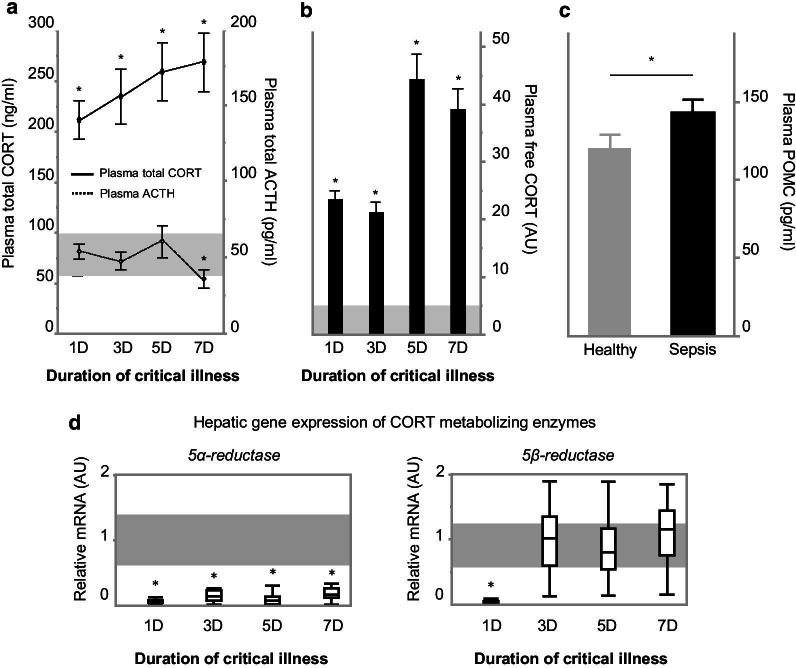
In two human studies of acute (ICU admission to day 7, N = 71) and prolonged (from ICU day 7 until recovery; N = 65) sepsis-induced critical illness, POMC plasma concentrations were quantified in relation to plasma ACTH and cortisol. In a mouse study of acute (1 day), subacute (3 and 5 days) and prolonged (7 days) fluid-resuscitated, antibiotic-treated sepsis (N = 123), we further documented alterations in hypothalamic CRH and AVP, plasma and pituitary POMC and its glucocorticoid-receptor-regulated processing into ACTH, as well as adrenal cortex integrity and steroidogenesis markers.
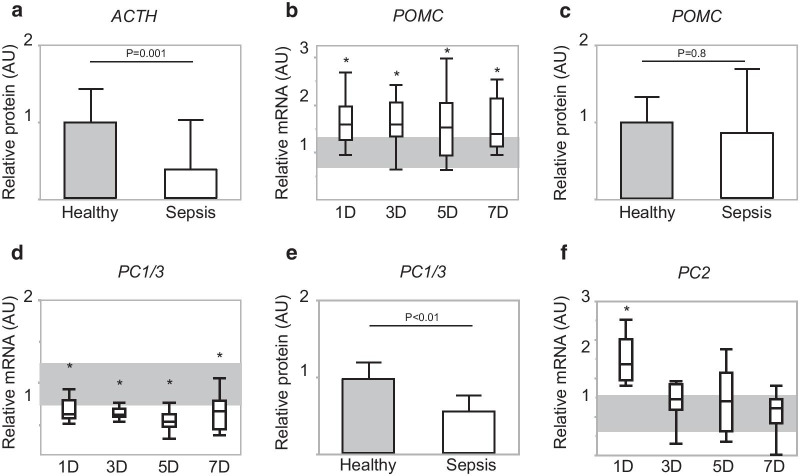
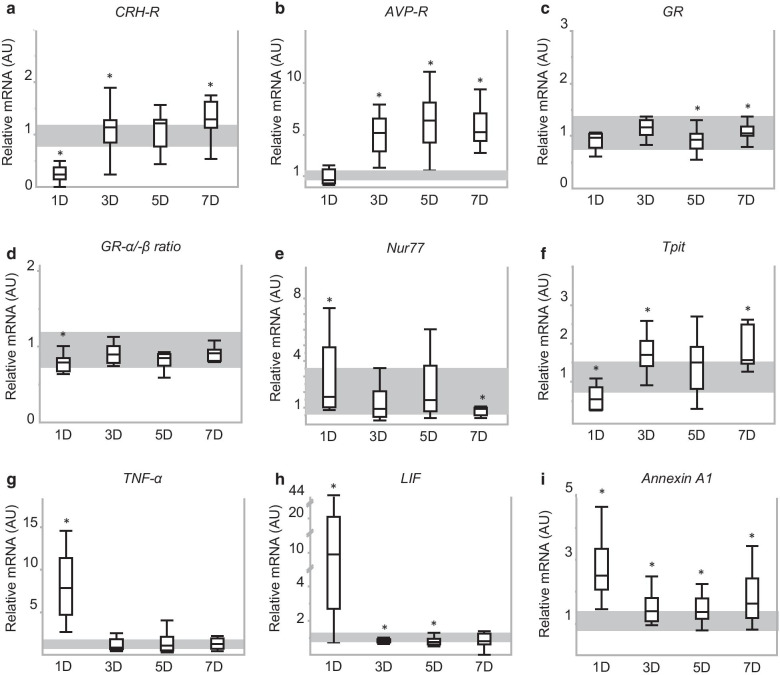
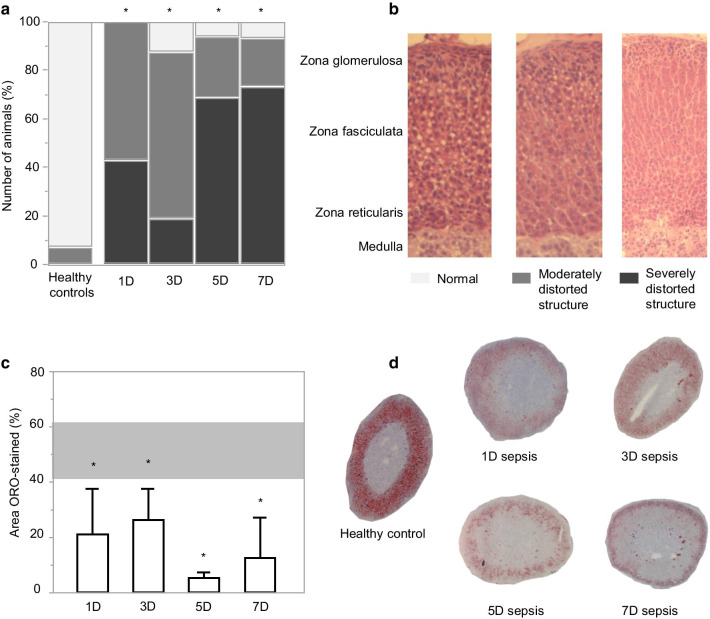
The two human studies revealed several-fold elevated plasma concentrations of the ACTH precursor POMC from the acute to the prolonged phase of sepsis and upon recovery (all p < 0.0001), coinciding with the known ACTH-cortisol dissociation. Elevated plasma POMC and ACTH-corticosterone dissociation were confirmed in the mouse model. In mice, sepsis acutely increased hypothalamic mRNA of CRH (p = 0.04) and AVP (p = 0.03) which subsequently normalized. From 3 days onward, pituitary expression of CRH receptor and AVP receptor was increased. From acute throughout prolonged sepsis, pituitary POMC mRNA was always elevated (all p < 0.05). In contrast, markers of POMC processing into ACTH and of ACTH secretion, negatively regulated by glucocorticoid receptor ligand binding, were suppressed at all time points (all p ≤ 0.05). Distorted adrenocortical structure (p < 0.05) and lipid depletion (p < 0.05) were present, while most markers of adrenocortical steroidogenic activity were increased at all time points (all p < 0.05).
Together, these findings suggest that increased circulating POMC, through CRH/AVP-driven POMC expression and impaired processing into ACTH, could represent a new piece in the puzzling ACTH-cortisol dissociation.
脓毒症的典型特征是血浆(游离)皮质醇升高和皮质醇分解抑制,而血浆促肾上腺皮质激素(ACTH)不增加,称为“ACTH-皮质醇分离”。我们假设脓毒症会激活下丘脑,通过促肾上腺皮质激素释放激素(CRH)和血管加压素(AVP)产生 ACTH 诱导的皮质醇增多症。此后,由于游离皮质醇的可用性增加,其分解减少,垂体水平的反馈抑制会干扰前阿黑皮素原(POMC)转化为 ACTH 的正常处理,从而解释了 ACTH-皮质醇分离。我们进一步假设,在这种情况下,POMC 会渗漏到循环中,并有助于肾上腺皮质类固醇的合成。
在两项关于急性(入住 ICU 至第 7 天,N=71)和延长(从 ICU 第 7 天到恢复;N=65)脓毒症诱导的危重病的人类研究中,我们定量检测了 POMC 血浆浓度与血浆 ACTH 和皮质醇的关系。在一项关于急性(1 天)、亚急性(3 天和 5 天)和延长(7 天)液体复苏、抗生素治疗的脓毒症(N=123)的小鼠研究中,我们进一步记录了下丘脑 CRH 和 AVP、血浆和垂体 POMC 及其糖皮质激素受体调节转化为 ACTH 的变化,以及肾上腺皮质完整性和类固醇生成标志物。
这两项人类研究表明,从脓毒症的急性到延长阶段以及恢复阶段,POMC(ACTH 的前体)的血浆浓度增加了数倍(均 p<0.0001),同时出现了已知的 ACTH-皮质醇分离。在小鼠模型中也证实了血浆 POMC 和 ACTH-皮质酮的分离。在小鼠中,脓毒症急性增加了下丘脑 CRH(p=0.04)和 AVP(p=0.03)的 mRNA,随后恢复正常。从第 3 天开始,垂体 CRH 受体和 AVP 受体的表达增加。从急性到延长的脓毒症,垂体 POMC mRNA 始终升高(均 p<0.05)。相比之下,调节 ACTH 分泌的 POMC 加工成 ACTH 的标志物以及受糖皮质激素受体配体结合负调节的 ACTH 分泌标志物在所有时间点均受到抑制(均 p≤0.05)。存在扭曲的肾上腺皮质结构(p<0.05)和脂质耗竭(p<0.05),而大多数肾上腺皮质类固醇生成活性标志物在所有时间点均增加(均 p<0.05)。
综上所述,这些发现表明,循环中 POMC 的增加,通过 CRH/AVP 驱动的 POMC 表达和受损的 ACTH 加工,可能代表了 ACTH-皮质醇分离的一个新谜团。