Department of Nephrology and Hypertension, Inselspital University Hospital Bern, Bern, Switzerland.
Department of Clinical Chemistry, Inselspital Universitatsspital Bern, Bern, Switzerland.
RMD Open. 2022 Mar;8(1). doi: 10.1136/rmdopen-2021-002166.
The majority of patients with B-cell-depleting therapies show compromised vaccination-induced immune responses. Herein, we report on the trajectories of anti-SARS-CoV-2 immune responses in patients of the RituxiVac study compared with healthy volunteers and investigate the immunogenicity of a third vaccination in previously humoral non-responding patients.
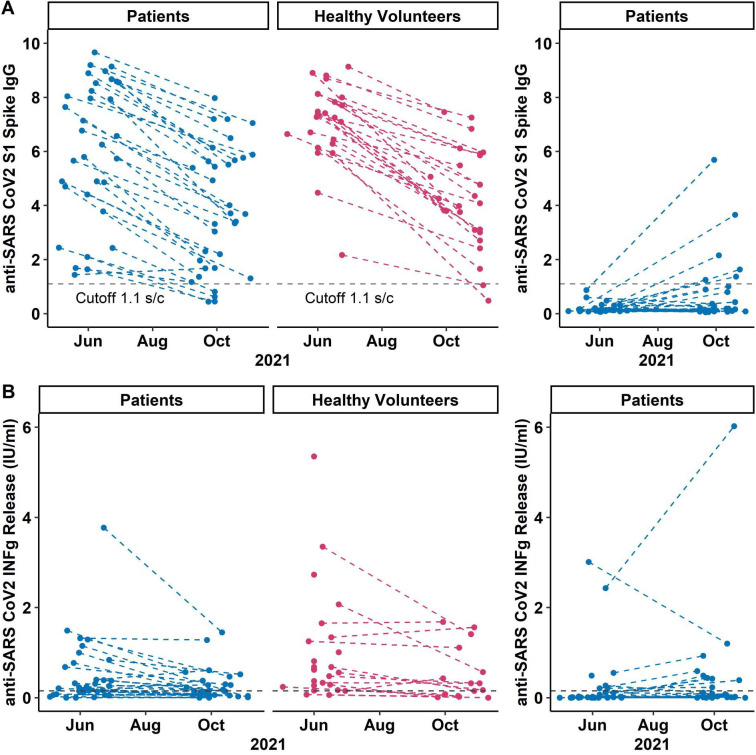
We investigated the humoral and cell-mediated immune response after SARS-CoV-2 messanger RNA vaccination in patients with a history with anti-CD20 therapies. Coprimary outcomes were antispike and SARS-CoV-2-stimulated interferon-γ concentrations in vaccine responders 4.3 months (median; IQR: 3.6-4.8 months) after first evaluation, and humoral and cell-mediated immunity (CMI) after a third vaccine dose in previous humoral non-responders. Immunity decay rates were compared using analysis of covariance in linear regression.
5.6 months (IQR: 5.1-6.7) after the second vaccination, we detected antispike IgG in 88% (29/33) and CMI in 44% (14/32) of patients with a humoral response after two-dose vaccination compared with 92% (24/26) healthy volunteers with antispike IgG and 69% (11/16) with CMI 6.8 months after the second vaccination (IQR: 6.0-7.1). Decay rates of antibody concentrations were comparable between patients and controls (p=0.70). In two-dose non-responders, a third SARS-CoV-2 vaccine elicited humoral responses in 19% (6/32) and CMI in 32% (10/31) participants.
This study reveals comparable immunity decay rates between patients with anti-CD20 treatments and healthy volunteers, but inefficient humoral or CMI after a third SARS-CoV-2 vaccine in most two-dose humoral non-responders calling for individually tailored vaccination strategies in this population.Trial registration numberNCT04877496; ClinicalTrials.gov number.
大多数接受 B 细胞耗竭治疗的患者表现出疫苗诱导的免疫反应受损。在此,我们报告了 RituxiVac 研究中患者的抗 SARS-CoV-2 免疫反应轨迹,并研究了既往体液无反应患者第三次接种疫苗的免疫原性。
我们研究了既往接受抗 CD20 治疗的患者在接受 SARS-CoV-2 信使 RNA 疫苗接种后的体液和细胞介导免疫反应。主要转归指标是初次评估后 4.3 个月(中位数;IQR:3.6-4.8 个月)时疫苗应答者的抗刺突和 SARS-CoV-2 刺激的干扰素-γ浓度,以及既往体液无应答者第三次疫苗接种后的体液和细胞介导免疫(CMI)。使用线性回归中的协方差分析比较免疫衰减率。
第二次接种后 5.6 个月(IQR:5.1-6.7),与第二次接种后 6.8 个月(IQR:6.0-7.1)时具有抗刺突 IgG 的 92%(24/26)健康志愿者和具有 CMI 的 69%(11/16)相比,我们在 2 剂疫苗接种后具有体液应答的 88%(29/33)患者中检测到抗刺突 IgG,在 44%(14/32)患者中检测到 CMI。患者和对照之间的抗体浓度衰减率无差异(p=0.70)。在 2 剂无应答者中,第三次 SARS-CoV-2 疫苗在 32%(10/31)的参与者中引发了体液反应,在 19%(6/32)的参与者中引发了 CMI。
这项研究表明,接受抗 CD20 治疗的患者与健康志愿者之间的免疫衰减率相当,但大多数 2 剂体液无应答者的第三次 SARS-CoV-2 疫苗接种后产生的体液或 CMI 效率较低,需要为该人群制定个体化的疫苗接种策略。
NCT04877496;临床试验编号:ClinicalTrials.gov 编号。