Lank Center for Genitourinary Oncology, Dana-Farber Cancer Institute, Boston, Massachusetts.
Florida Cancer Specialists and Research Institute/Sarah Cannon Research Institute, Port Charlotte, Florida.
Clin Cancer Res. 2022 Jun 1;28(11):2237-2247. doi: 10.1158/1078-0432.CCR-21-2326.
To report efficacy and safety of samotolisib (LY3023414; PI3K/mTOR dual kinase and DNA-dependent protein kinase inhibitor) plus enzalutamide in patients with metastatic castration-resistant prostate cancer (mCRPC) following cancer progression on abiraterone.
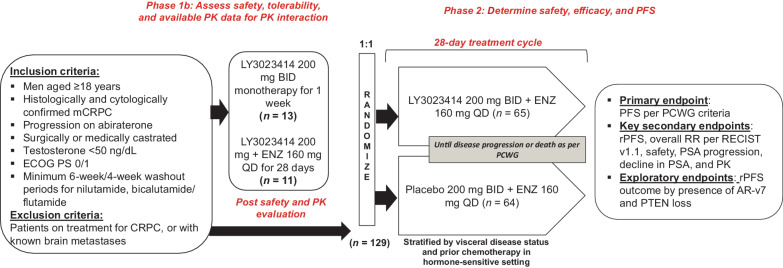
In this double-blind, placebo-controlled phase Ib/II study (NCT02407054), following a lead-in segment for evaluating safety and pharmacokinetics of samotolisib and enzalutamide combination, patients with advanced castration-resistant prostate cancer with progression on prior abiraterone were randomized to receive enzalutamide (160 mg daily)/samotolisib (200 mg twice daily) or placebo. Primary endpoint was progression-free survival (PFS) assessed by Prostate Cancer Clinical Trials Working Group criteria (PCWG2). Secondary and exploratory endpoints included radiographic PFS (rPFS) and biomarkers, respectively. Log-rank tests assessed treatment group differences.
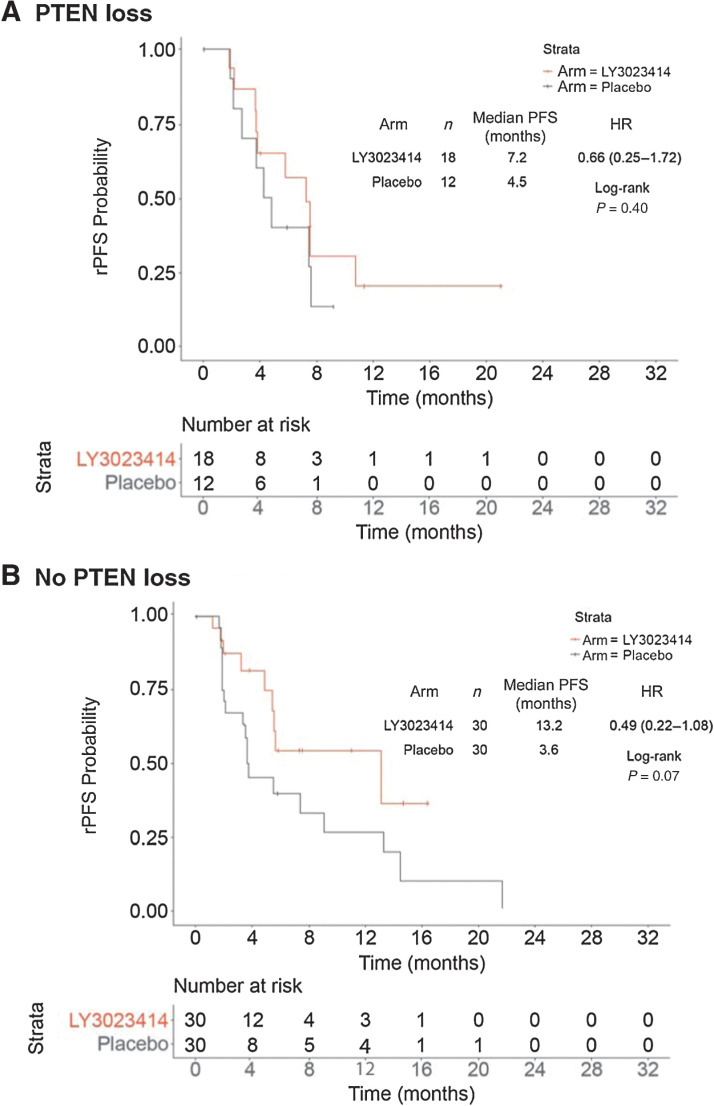
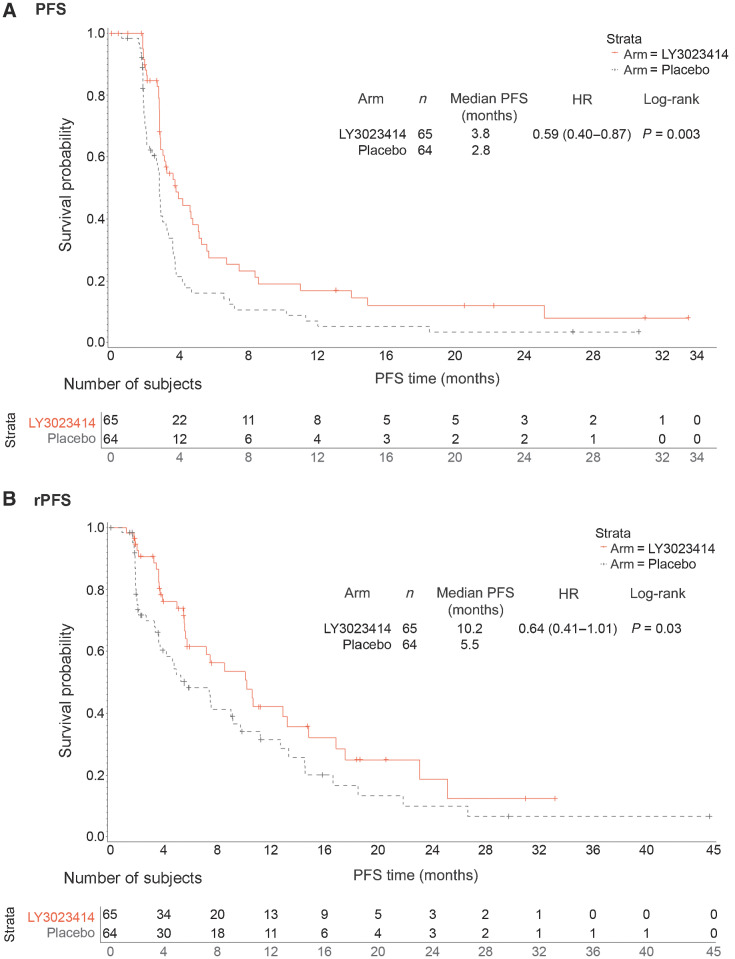
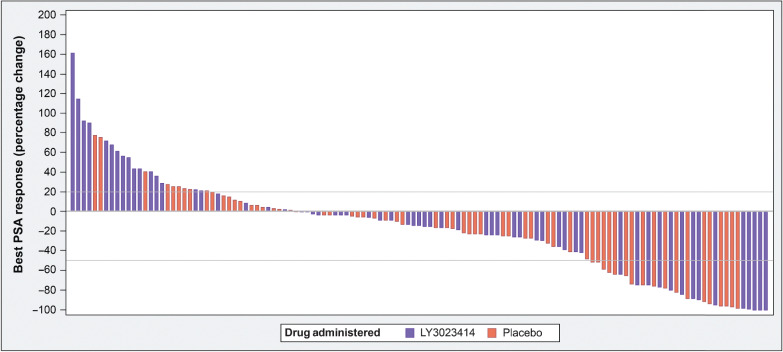
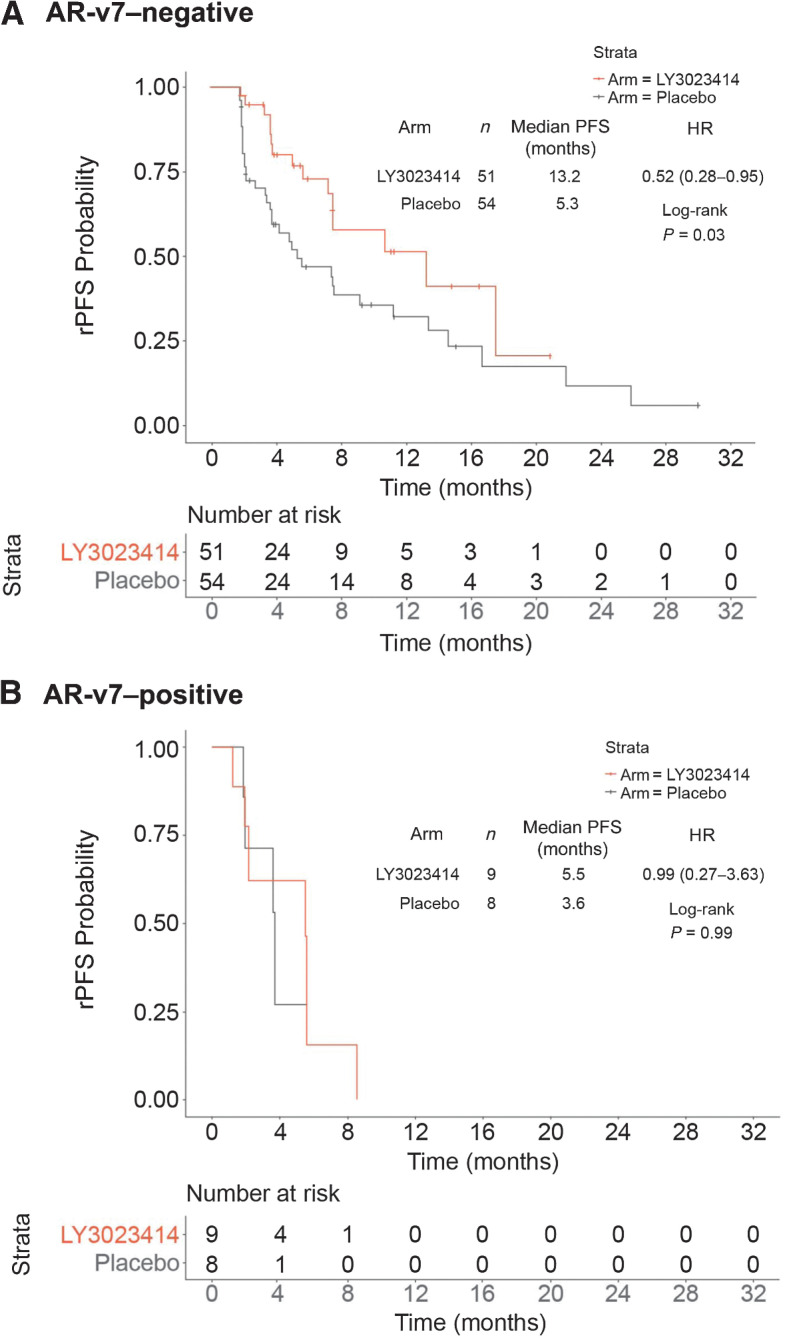
Overall, 13 and 129 patients were enrolled in phase Ib and II, respectively. Dose-limiting toxicity was not reported in patients during phase Ib and mean samotolisib exposures remained in the targeted range despite a 35% decrease when administered with enzalutamide. In phase II, median PCWG2-PFS and rPFS was significantly longer in the samotolisib/enzalutamide versus placebo/enzalutamide arm (3.8 vs. 2.8 months; P = 0.003 and 10.2 vs. 5.5 months; P = 0.03), respectively. Patients without androgen receptor splice variant 7 showed a significant and clinically meaningful rPFS benefit in the samotolisib/enzalutamide versus placebo/enzalutamide arm (13.2 months vs. 5.3 months; P = 0.03).
Samotolisib/enzalutamide has tolerable side effects and significantly improved PFS in patients with mCRPC with cancer progression on abiraterone, and this may be enriched in patients with PTEN intact and no androgen receptor splice variant 7.
报告索拉非尼(LY3023414;PI3K/mTOR 双重激酶和 DNA 依赖性蛋白激酶抑制剂)联合恩扎卢胺在先前接受阿比特龙治疗后发生进展的转移性去势抵抗性前列腺癌(mCRPC)患者中的疗效和安全性。
在这项双盲、安慰剂对照的 Ib/II 期研究(NCT02407054)中,在评估索拉非尼和恩扎卢胺联合用药安全性和药代动力学的先导段后,先前接受阿比特龙治疗后发生进展的晚期去势抵抗性前列腺癌患者被随机分配接受恩扎卢胺(每日 160mg)/索拉非尼(每日 2 次,每次 200mg)或安慰剂。主要终点是根据前列腺癌临床试验工作组标准(PCWG2)评估的无进展生存期(PFS)。次要和探索性终点分别为放射学无进展生存期(rPFS)和生物标志物。对数秩检验评估了治疗组之间的差异。
总体而言,Ib 期和 II 期分别有 13 例和 129 例患者入组。Ib 期患者未报告剂量限制毒性,尽管与恩扎卢胺联合应用时暴露量减少了 35%,但索拉非尼的平均暴露量仍在目标范围内。在 II 期,索拉非尼/恩扎卢胺组与安慰剂/恩扎卢胺组的中位 PCWG2-PFS 和 rPFS 显著延长(分别为 3.8 个月 vs. 2.8 个月;P = 0.003 和 10.2 个月 vs. 5.5 个月;P = 0.03)。无雄激素受体剪接变异体 7 的患者在索拉非尼/恩扎卢胺组与安慰剂/恩扎卢胺组的 rPFS 获益具有显著且有临床意义(13.2 个月 vs. 5.3 个月;P = 0.03)。
索拉非尼/恩扎卢胺耐受性良好,可显著改善先前接受阿比特龙治疗后发生进展的 mCRPC 患者的 PFS,且在 PTEN 完整且无雄激素受体剪接变异体 7 的患者中可能更为显著。