Department of Neurosurgery, Neurosciences, and Neurology, University of New Mexico, NM, Albuquerque, USA.
Department of Internal Medicine, University of New Mexico, Albuquerque, NM, USA.
Transl Stroke Res. 2023 Apr;14(2):160-173. doi: 10.1007/s12975-022-01014-7. Epub 2022 Apr 2.
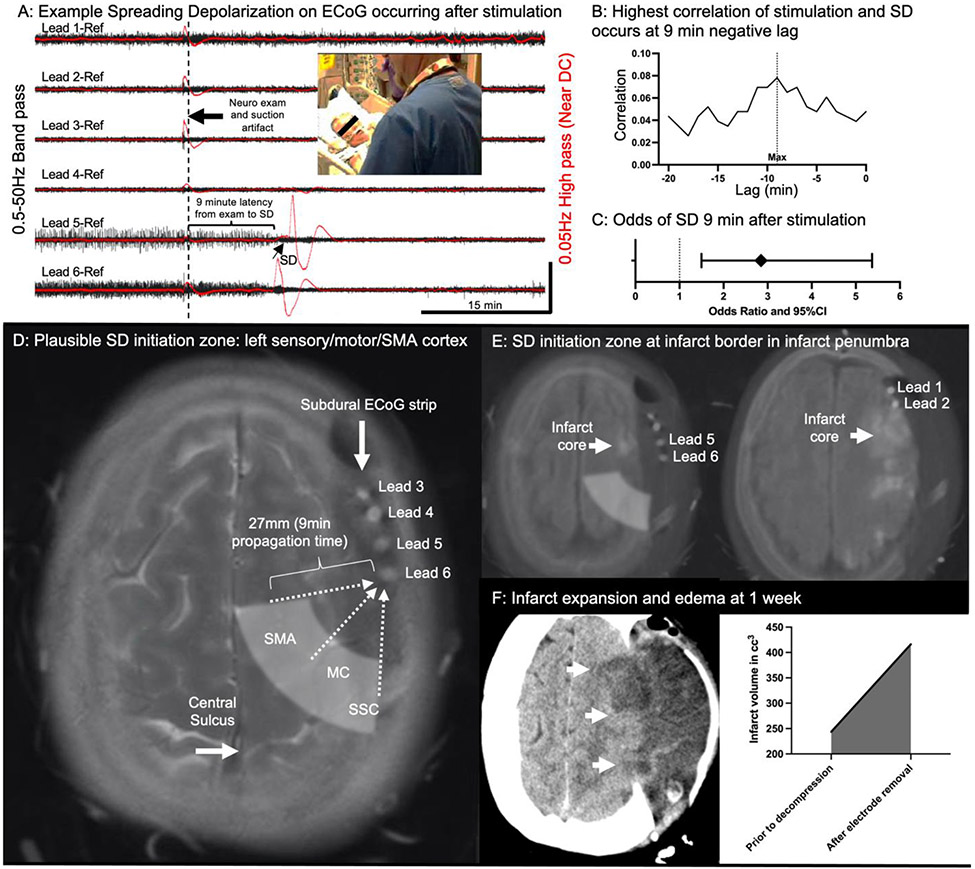
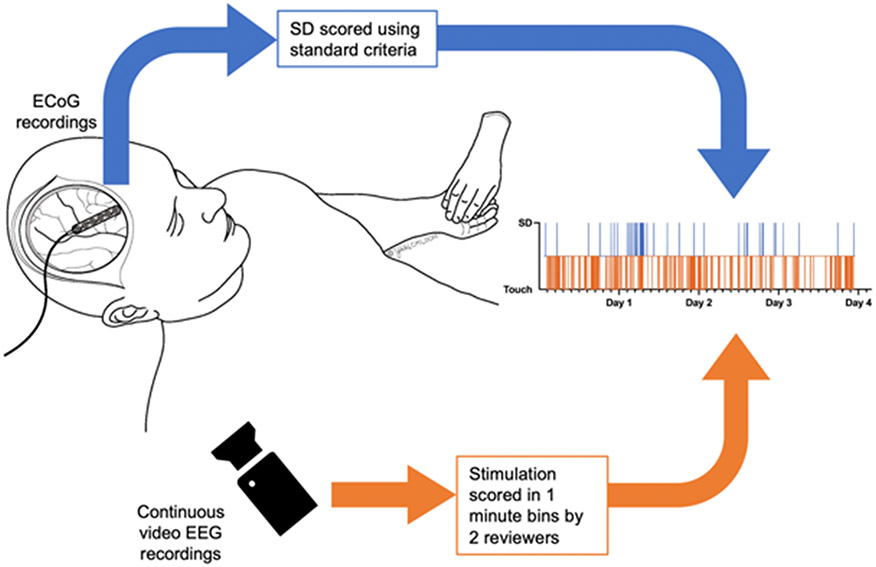
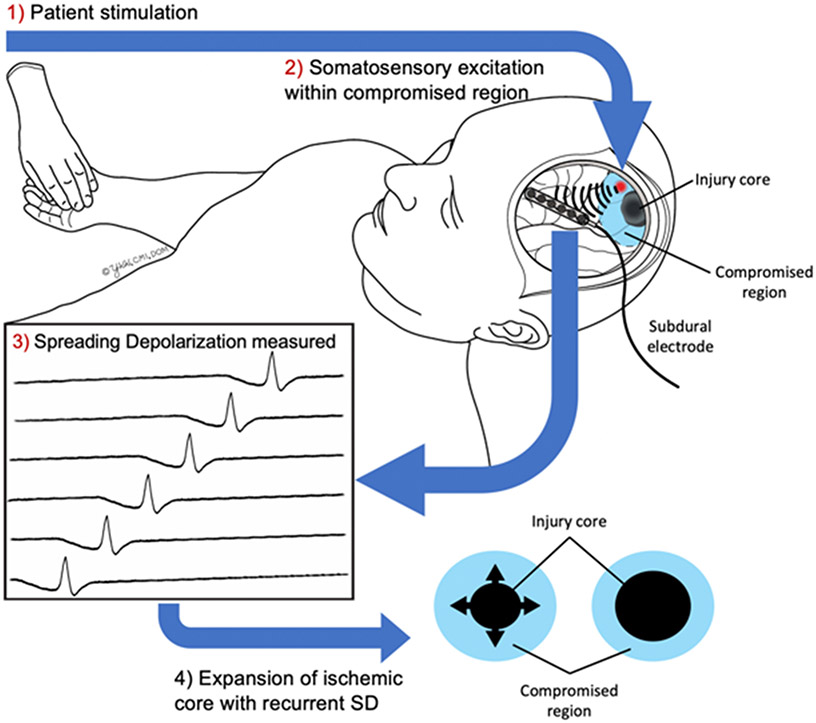
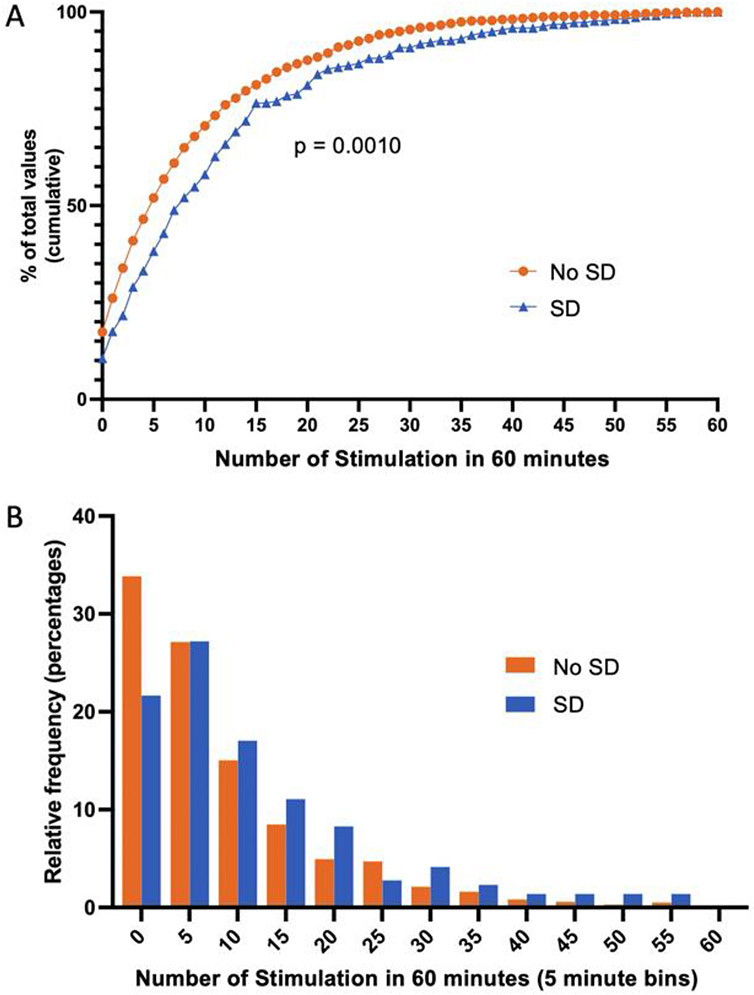
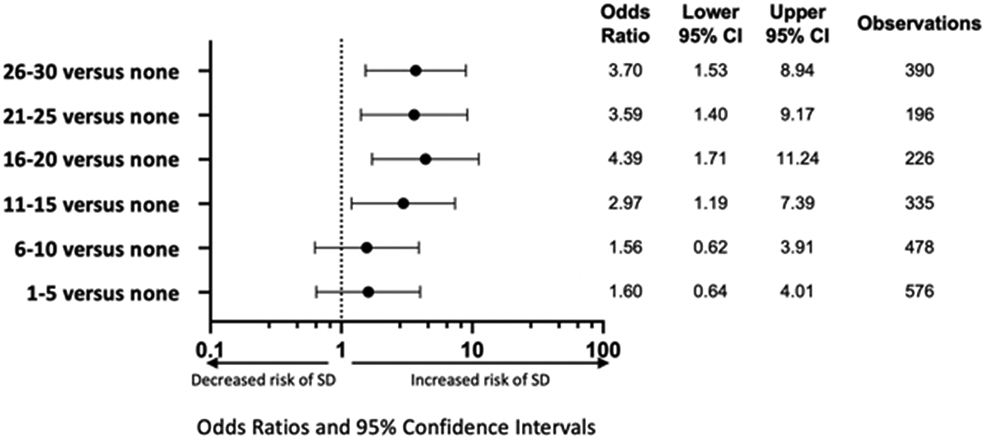
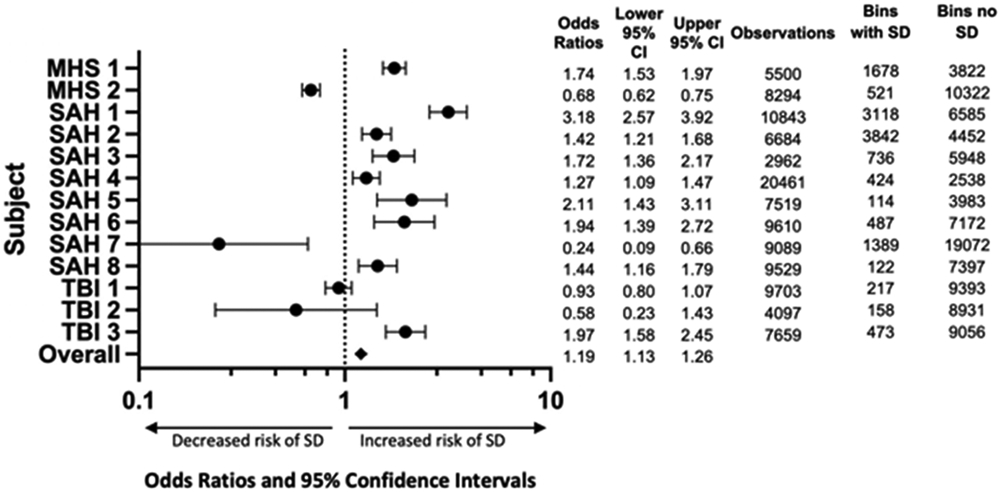
Touch and other types of patient stimulation are necessary in critical care and generally presumed to be beneficial. Recent pre-clinical studies as well as randomized trials assessing early mobilization have challenged the safety of such routine practices in patients with acute neurological injury such as stroke. We sought to determine whether patient stimulation could result in spreading depolarization (SD), a dramatic pathophysiological event that likely contributes to metabolic stress and ischemic expansion in such patients. Patients undergoing surgical intervention for severe acute neurological injuries (stroke, aneurysm rupture, or trauma) were prospectively consented and enrolled in an observational study monitoring SD with implanted subdural electrodes. Subjects also underwent simultaneous video recordings (from continuous EEG monitoring) to assess for physical touch and other forms of patient stimulation (such as suctioning and positioning). The association of patient stimulation with subsequent SD was assessed. Increased frequency of patient stimulation was associated with increased risk of SD (OR = 4.39 [95%CI = 1.71-11.24]). The overall risk of SD was also increased in the 60 min following patient stimulation compared to times with no stimulation (OR = 1.19 [95%CI = 1.13-1.26]), though not all subjects demonstrated this effect individually. Positioning of the subject was the subtype of stimulation with the strongest overall effect on SD (OR = 4.92 [95%CI = 3.74-6.47]). We conclude that in patients with some acute neurological injuries, touch and other patient stimulation can induce SD (PS-SD), potentially increasing the risk of metabolic and ischemic stress. PS-SD may represent an underlying mechanism for observed increased risk of early mobilization in such patients.
在重症监护中,触摸和其他类型的患者刺激是必要的,通常被认为是有益的。最近的临床前研究以及评估早期活动的随机试验挑战了急性神经损伤(如中风)患者此类常规操作的安全性。我们试图确定患者刺激是否会导致扩散性去极化(SD),这是一种可能导致此类患者代谢应激和缺血扩大的剧烈病理生理事件。我们前瞻性地同意并招募了正在接受手术干预的严重急性神经损伤(中风、动脉瘤破裂或创伤)患者,进行了一项观察性研究,通过植入的硬脑膜下电极监测 SD。患者还接受了同步视频记录(来自连续 EEG 监测),以评估身体触摸和其他形式的患者刺激(如吸引和定位)。评估了患者刺激与随后的 SD 之间的关联。患者刺激频率的增加与 SD 的风险增加相关(OR=4.39 [95%CI=1.71-11.24])。与无刺激相比,在刺激后 60 分钟内 SD 的总体风险也增加(OR=1.19 [95%CI=1.13-1.26]),尽管并非所有患者个体都表现出这种效应。与其他刺激类型相比,患者体位改变对 SD 的总体影响最强(OR=4.92 [95%CI=3.74-6.47])。我们得出结论,在一些急性神经损伤患者中,触摸和其他患者刺激可诱发 SD(PS-SD),可能会增加代谢和缺血应激的风险。PS-SD 可能代表了此类患者早期活动增加风险的潜在机制。