Maidstone and Tunbridge Wells NHS Trust, Tunbridge Wells, UK.
Institute of Medical Sciences, Christ Church Canterbury University, Kent, UK.
BMC Ophthalmol. 2022 Apr 2;22(1):152. doi: 10.1186/s12886-022-02361-7.
Treatment of open angle glaucoma (OAG) and/or ocular hypertension (OHT) focuses on achievement of target intraocular pressure (IOP), with the objective of slowing disease progression. However, ocular surface health is an important consideration in the optimization of treatment. We report 6 patient cases in which enhanced IOP control was achieved following appropriate management of ocular surface inflammation and a therapeutic switch to the preservative-free (PF) tafluprost (0.0015%)/timolol (0.5%) fixed-dose combination (FC).
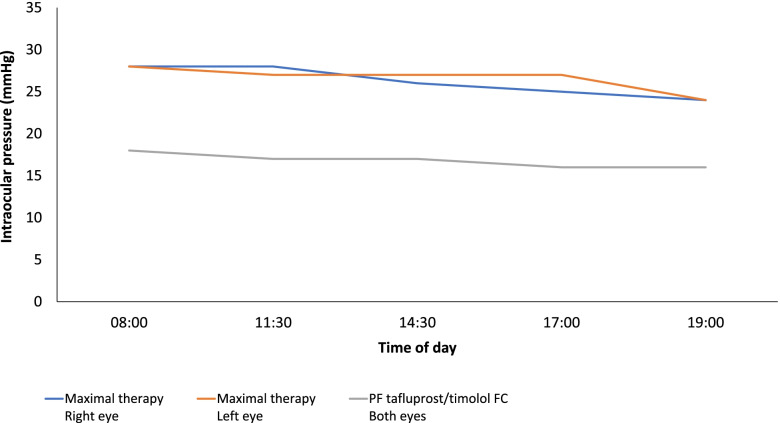
Six patient cases, aged 48-74 years, presented with OAG or OHT. Each patient had signs and symptoms of ocular surface disease (OSD). Cases 1-3 were each receiving maximal medical therapy for OAG; regimens comprising prostaglandin analogue (PGA), β-blocker, carbonic anhydrase inhibitor (CAI) and α-2 agonist agents (including treatments containing preservative agent). Cases 1 and 2 reported IOP values ≥23 mmHg in each eye, and wide IOP fluctuations were identified when reviewing patient data concerning case 3 (11-20 mmHg). Maximal therapy was ceased and PF tafluprost/timolol FC was initiated, after which the signs and symptoms of OSD were improved and IOP was reduced (≤18 mmHg for cases 1-3) and stabilized. Cases 4 and 5 were diagnosed with OAG and case 6 had OHT. Each had symptoms and signs of OSD and were treated with a preserved PGA monotherapy (latanoprost 0.005% or bimatoprost 0.03%). At presentation, IOP was 24 mmHg in both eyes (case 4), ≥18 mmHg (case 5) and ≥ 22 mmHg (case 6). Following a switch to the PF tafluprost/timolol FC, OSD symptoms were improved and IOP was 14 mmHg (both eyes; case 4), ≤14 mmHg (case 5) and 16 mmHg (both eyes; case 6).
In addition to IOP-lowering efficacy, approaches to the management of OAG and OHT should consider the impact of treatment tolerability and the susceptibility of these patients to OSD. The presence of ocular surface inflammation appears to be detrimental to adherence and therefore to the effectiveness of topical medications. Addressing OSD through the use of PF FC formations, such as the PF tafluprost/timolol FC, reduces exposure to potentially toxic agents and facilitates improvements in IOP control.
开角型青光眼(OAG)和/或高眼压症(OHT)的治疗侧重于达到目标眼压(IOP),目的是减缓疾病进展。然而,眼表面健康是优化治疗的一个重要考虑因素。我们报告了 6 例患者的病例,这些患者在适当治疗眼表面炎症和从含防腐剂的他氟前列素(0.0015%)/噻吗洛尔(0.5%)固定剂量组合(FC)治疗转换后,实现了增强的 IOP 控制。
6 例患者,年龄 48-74 岁,患有 OAG 或 OHT。每位患者均有眼表面疾病(OSD)的体征和症状。病例 1-3 均接受了 OAG 的最大药物治疗;方案包括前列腺素类似物(PGA)、β-阻滞剂、碳酸酐酶抑制剂(CAI)和α-2 激动剂(包括含防腐剂的治疗)。病例 1 和 2 报告说每只眼的 IOP 值均≥23mmHg,当回顾病例 3 的患者数据时,发现 IOP 波动较大(11-20mmHg)。停止最大治疗后,开始使用 PF 他氟前列素/噻吗洛尔 FC,此后 OSD 的体征和症状得到改善,IOP 降低(病例 1-3 均≤18mmHg)并稳定。病例 4 和 5 被诊断为 OAG,病例 6 患有 OHT。他们均有 OSD 的症状和体征,并接受了含防腐剂的 PGA 单一疗法(拉坦前列素 0.005%或贝美前列素 0.03%)治疗。就诊时,病例 4 双眼的 IOP 均为 24mmHg,病例 5 的 IOP≥18mmHg,病例 6 的 IOP≥22mmHg。在改用 PF 他氟前列素/噻吗洛尔 FC 后,OSD 症状得到改善,IOP 为 14mmHg(双眼;病例 4)、≤14mmHg(病例 5)和 16mmHg(双眼;病例 6)。
除了降低 IOP 的效果外,OAG 和 OHT 的治疗方法还应考虑治疗耐受性的影响以及这些患者对 OSD 的易感性。眼表面炎症的存在似乎对依从性不利,因此对局部药物的有效性不利。通过使用 PF FC 制剂(如 PF 他氟前列素/噻吗洛尔 FC)来解决 OSD,可以减少接触潜在毒性物质,并有助于改善 IOP 控制。