Leong Kai'En, Howard Luke, Lo Giudice Francesco, Pavey Holly, Davies Rachel, Haji Gulammehdi, Gibbs Simon, Gopalan Deepa
Department of Radiology, Imperial College National Health Service Trust/Hammersmith Hospital, London, United Kingdom.
Department of Cardiology, The Royal Melbourne Hospital, Parkville, VIC, Australia.
Front Cardiovasc Med. 2022 Mar 17;9:787656. doi: 10.3389/fcvm.2022.787656. eCollection 2022.
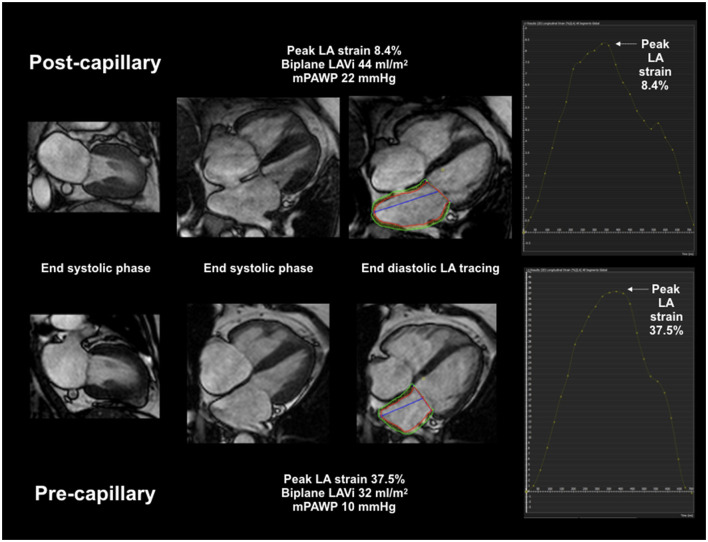
Pulmonary hypertension (PH) is dichotomized into pre- and post-capillary physiology by invasive catheterization. Imaging, particularly strain assessment, may aid in classification and be helpful with ambiguous hemodynamics. We sought to define cardiac MRI (CMR) feature tracking biatrial peak reservoir and biventricular peak systolic strain in pre- and post-capillary PH and examine the performance of peak left atrial strain in distinguishing the 2 groups compared to TTE.
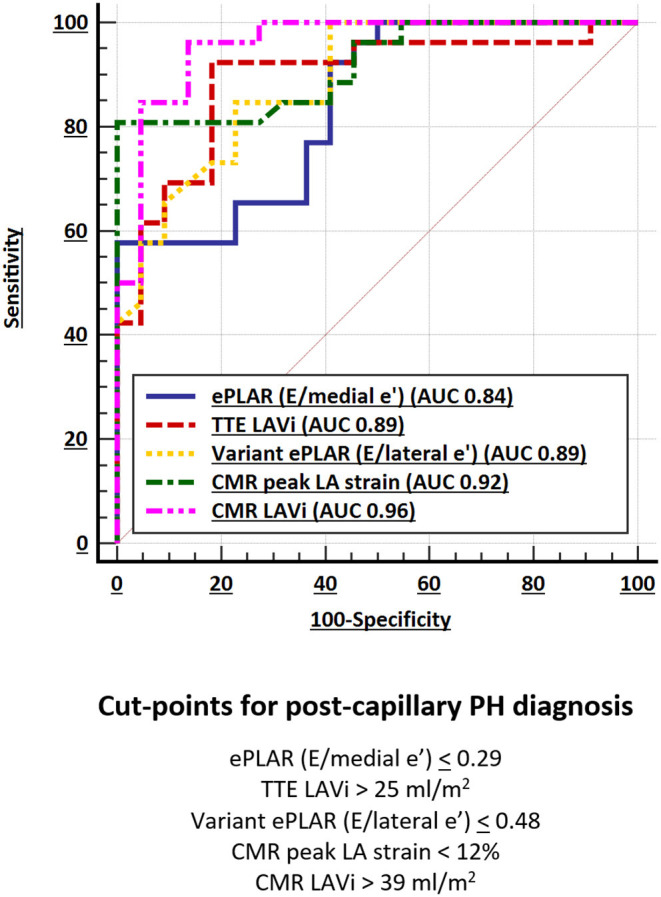
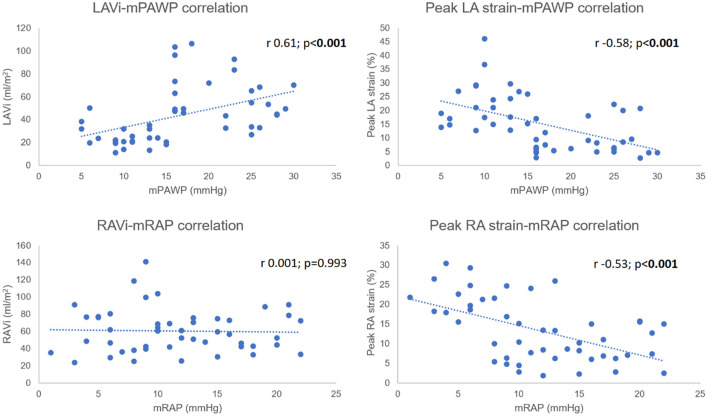
Retrospective cross-sectional study from 1 Jan 2015 to 31 Dec 2020; 48 patients (22 pre- and 26 post-capillary) were included with contemporaneous TTE, CMR and catheterization. Mean pulmonary artery pressures were higher in the pre-capillary cohort (55 ± 14 vs. 42 ± 9 mmHg; < 0.001) as was pulmonary vascular resistance (median 11.7 vs. 3.7 WU; < 0.001). Post-capillary patients had significantly larger left atria (60 ± 22 vs. 25 ± 9 ml/m; < 0.001). There was no difference in right atrial volumes between groups (60 ± 21 vs. 61 ± 29 ml/m; = 0.694), however peak RA strain was lower in post-capillary PH patients (8.9 ± 5.5 vs. 18.8 ± 7.0%; < 0.001). In the post-capillary group, there was commensurately severe peak strain impairment in both atria (LA strain 9.0 ± 5.8%, RA strain 8.9 ± 5.5%). CMR LAVi and peak LA strain had a multivariate AUC of 0.98 (95% CI 0.89-1.00; < 0.001) for post-capillary PH diagnosis which was superior to TTE.
CMR volumetric and deformation assessment of the left atrium can highly accurately distinguish post- from pre-capillary PH.
通过有创导管检查将肺动脉高压(PH)分为毛细血管前和毛细血管后生理类型。影像学检查,尤其是应变评估,可能有助于分类,并有助于解决血流动力学不明确的问题。我们试图确定心脏磁共振成像(CMR)特征追踪的双房峰值储备和双心室峰值收缩应变在毛细血管前和毛细血管后PH中的情况,并与经胸超声心动图(TTE)比较,研究左房峰值应变在区分这两组中的表现。
对2015年1月1日至2020年12月31日进行回顾性横断面研究;纳入48例患者(22例毛细血管前和26例毛细血管后),同期进行TTE、CMR和导管检查。毛细血管前队列的平均肺动脉压较高(55±14 vs. 42±9 mmHg;P<0.001),肺血管阻力也较高(中位数11.7 vs. 3.7 WU;P<0.001)。毛细血管后患者的左心房明显更大(60±22 vs. 25±9 ml/m²;P<0.001)。两组间右心房容积无差异(60±21 vs. 61±29 ml/m²;P = 0.694),然而毛细血管后PH患者的右房峰值应变较低(8.9±5.5 vs. 18.8±7.0%;P<0.001)。在毛细血管后组中,两个心房的峰值应变均有相应的严重受损(左房应变9.0±5.8%,右房应变8.9±5.5%)。CMR左房容积指数(LAVi)和左房峰值应变在诊断毛细血管后PH时的多变量曲线下面积(AUC)为0.98(95%可信区间0.89 - 1.00;P<0.001),优于TTE。
CMR对左心房的容积和变形评估能够高度准确地区分毛细血管后与毛细血管前PH。