Virology Laboratory, Institute of Biological Sciences, Federal University of Pará, Belém, Brazil.
Epstein-Barr Virus Laboratory, Virology Unit, Evandro Chagas Institute, Ananindeua, Brazil.
Front Immunol. 2022 Mar 16;13:829126. doi: 10.3389/fimmu.2022.829126. eCollection 2022.
Immune reconstitution failure after HIV treatment is a multifactorial phenomenon that may also be associated with a single polymorphism of human leukocyte antigen (HLA); however, few reports include patients from the Brazilian Amazon. Our objective was to evaluate the association of the immunogenic profile of the "classical" HLA-I and HLA-II loci with treatment nonresponse in a regional cohort monitored over 24 months since HIV diagnosis.
Treatment-free participants from reference centers in the state of Pará, Brazil, were enrolled. Infection screening was performed using enzyme immunoassays (Murex AG/AB Combination DiaSorin, UK) and confirmed by immunoblots (Bio-Manguinhos, FIOCRUZ). Plasma viral load was quantified by real-time PCR (ABBOTT, Chicago, Illinois, USA). CD4/CD8 T lymphocyte quantification was performed by immunophenotyping and flow cytometry (BD Biosciences, San Jose, CA, USA). Infection was monitored test and logistics platforms (SISCEL and SICLOM). Therapeutic response failure was inferred based on CD4 T lymphocyte quantification after 1 year of therapy. Loci A, B and DRB1 were genotyped using PCR-SSO (One Lambda Inc., Canoga Park, CA, USA). Statistical tests were applied using GENEPOP, GraphPad Prism 8.4.3 and BioEstat 5.3.
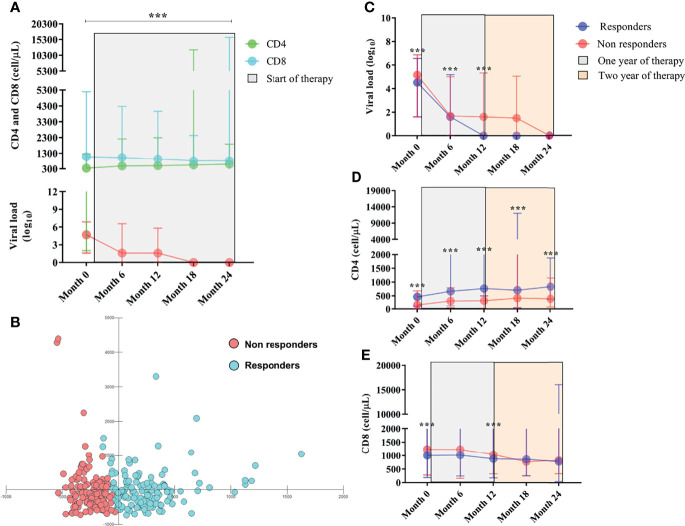
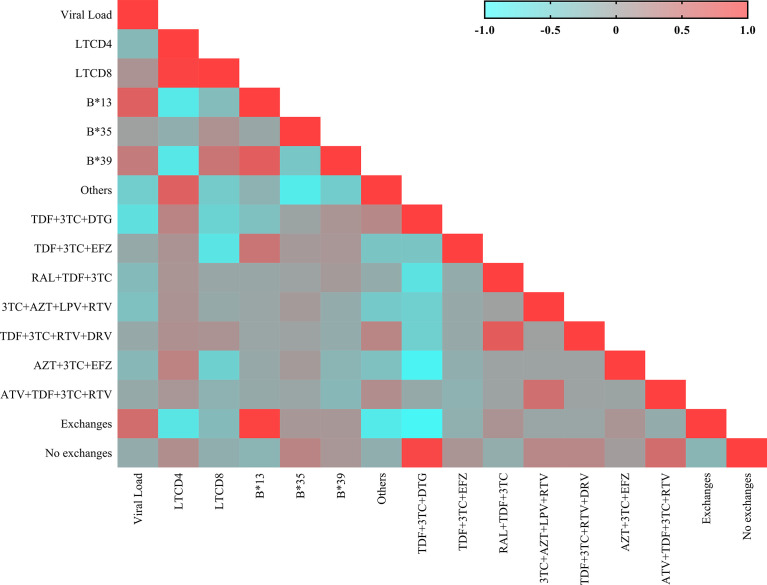
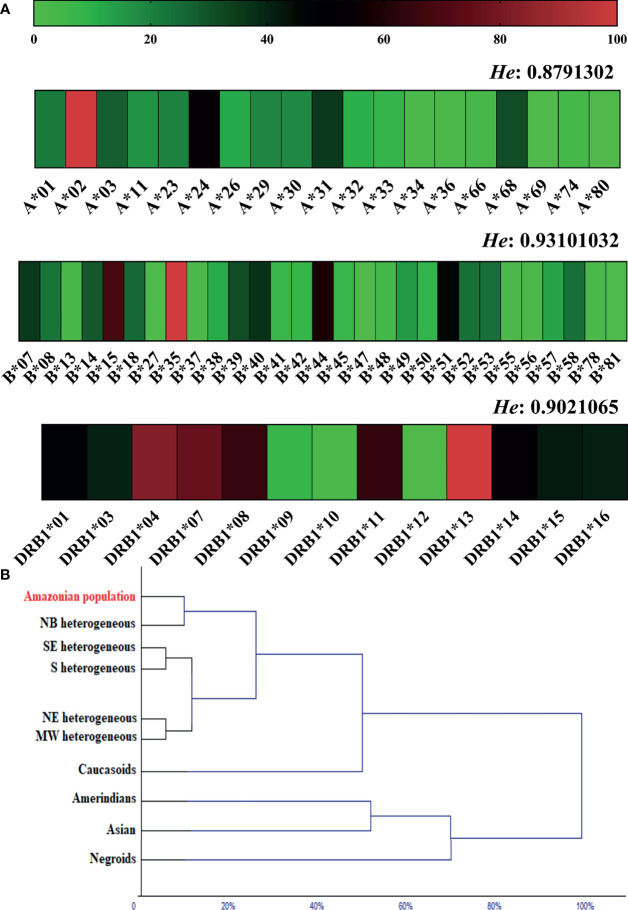
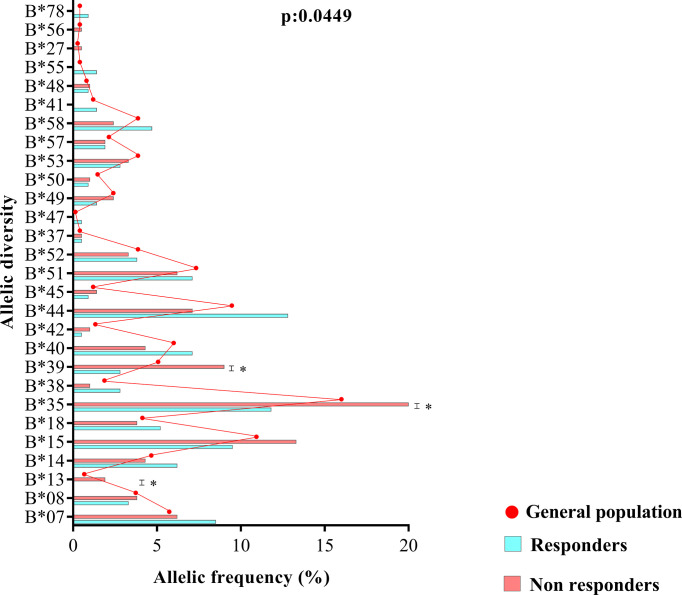
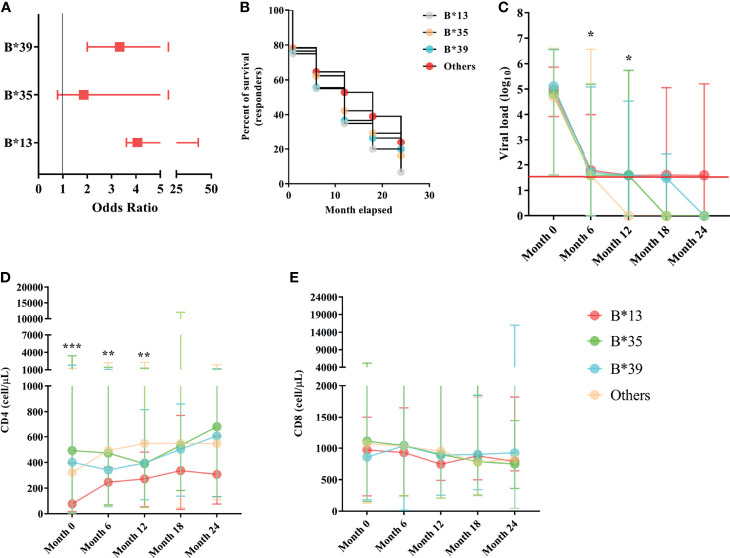
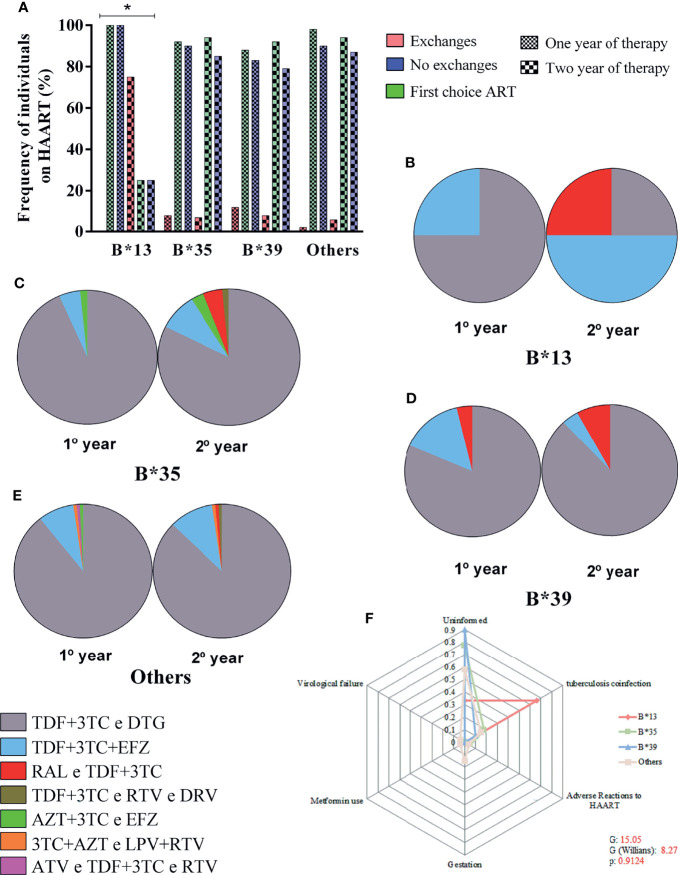
Of the 270 patients monitored, 134 responded to treatment (CD4 ≥ 500 cells/µL), and 136 did not respond to treatment (CD4 < 500 cells/µL). The allele frequencies of the loci were similar to heterogeneous populations. The allelic profile of locus B was statistically associated with treatment nonresponse, and the B13, B35 and B39 alleles had the greatest probabilistic influence. The B13 allele had the highest risk of treatment nonresponse, and carriers of the allele had a detectable viral load and a CD4+ T lymphocyte count less than 400 cells/µL with up to 2 years of therapy. The B*13 allele was associated with a switch in treatment regimens, preferably to efavirenz (EFZ)-based regimens, and among those who switched regimens, half had a history of coinfection with tuberculosis.
The allelic variants of the B locus are more associated with non-response to therapy in people living with HIV (PLHIV) from a heterogeneous population in the Brazilian Amazon.
艾滋病毒治疗后免疫重建失败是一种多因素现象,也可能与人类白细胞抗原(HLA)的单一多态性有关;然而,很少有报告包括来自巴西亚马逊地区的患者。我们的目的是评估“经典”HLA-I 和 HLA-II 基因座的免疫原性谱与艾滋病毒诊断后 24 个月内监测的区域队列中治疗无反应的相关性。
我们招募了来自巴西帕拉州参考中心的无治疗参与者。使用酶免疫测定法(Murex AG/AB 组合 DiaSorin,英国)进行感染筛查,并通过免疫印迹法(Bio-Manguinhos,FIOCRUZ)进行确认。通过实时 PCR(美国芝加哥的 ABBOTT)定量检测血浆病毒载量。通过免疫表型和流式细胞术(BD Biosciences,加利福尼亚州圣何塞)定量 CD4/CD8 T 淋巴细胞。使用 SISCEL 和 SICLOM 测试和物流平台进行感染监测。根据治疗 1 年后 CD4 T 淋巴细胞的定量推断治疗反应失败。使用 PCR-SSO(加利福尼亚州卡诺加帕克的 One Lambda Inc.)对 A、B 和 DRB1 基因座进行基因分型。使用 GENEPOP、GraphPad Prism 8.4.3 和 BioEstat 5.3 应用统计检验。
在监测的 270 名患者中,134 名对治疗有反应(CD4≥500 个细胞/µL),136 名对治疗无反应(CD4<500 个细胞/µL)。基因座的等位基因频率与异质人群相似。B 基因座的等位基因谱与治疗无反应呈统计学相关,B13、B35 和 B39 等位基因具有最大的概率影响。B13 等位基因具有最高的治疗无反应风险,携带该等位基因的患者在长达 2 年的治疗中具有可检测的病毒载量和低于 400 个细胞/µL 的 CD4+T 淋巴细胞计数。B*13 等位基因与治疗方案的转换相关,优选基于依非韦伦(EFZ)的方案,在转换方案的患者中,有一半人有结核病合并感染的病史。
在来自巴西亚马逊地区异质人群的艾滋病毒感染者(PLHIV)中,B 基因座的等位基因变体与治疗无反应的相关性更高。