Faust Hilary E, Oniyide Oluwatosin, Wang Yiyue, Forker Caitlin M, Dunn Thomas, Yang Wei, Lanken Paul N, Sims Carrie A, Yehya Nadir, Christie Jason D, Meyer Nuala J, Reilly John P, Mangalmurti Nilam S, Shashaty Michael G S
Division of Allergy, Pulmonary and Critical Care, Department of Medicine, University of Wisconsin School of Medicine and Public Health, Madison, WI.
Division of Pulmonary, Allergy and Critical Care, Department of Medicine, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA.
Crit Care Explor. 2022 Mar 28;4(4):e0663. doi: 10.1097/CCE.0000000000000663. eCollection 2022 Apr.
Circulating nucleic acids, alone and in complex with histones as nucleosomes, have been proposed to link systemic inflammation and coagulation after trauma to acute kidney injury (AKI). We sought to determine the association of circulating nucleic acids measured at multiple time points after trauma with AKI risk.
We conducted a prospective cohort study of trauma patients, collecting plasma on presentation and at 6, 12, 24, and 48 hours, defining AKI over the first 6 days by Kidney Disease Improving Global Outcomes serum creatinine and dialysis criteria. We determined kinetics of plasma mitochondrial DNA (mtDNA), nuclear DNA (nDNA), and nucleosome levels across time points and associations with AKI using multivariable linear mixed-effects models, adjusted for injury characteristics and blood transfusions. We evaluated the association of presentation nucleic acid damage-associated molecular patterns (DAMP) concentrations with subsequent AKI, adjusting for injury severity using multivariable logistic regression.
Academic level I trauma center.
Trauma patients ( = 55) requiring intensive care for greater than or equal to 24 hours after presentation.
None.
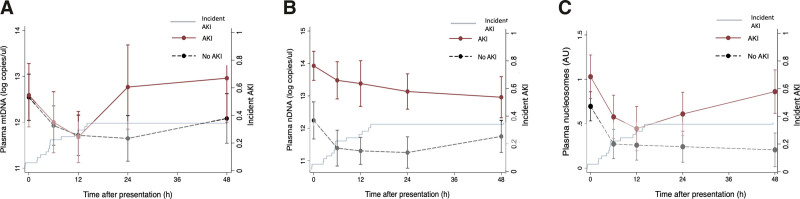
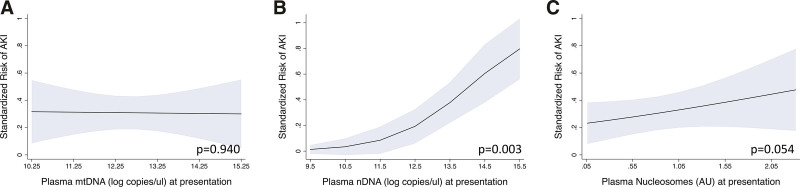
AKI developed in 17 patients (31%), a median of 12.0 hours (interquartile range, 6.2-24.1 hr) after presentation. mtDNA demonstrated a time-varying association with AKI ( = 0.022, interaction with time point), with differences by AKI status not emerging until 24 hours (β = 0.97 [95% CI, 0.03-1.90] log copies/uL; = 0.043). Patients who developed AKI had higher nDNA across all time points (overall β = 1.41 log copies/uL [0.86-1.95 log copies/uL]; < 0.001), and presentation levels were significantly associated with subsequent AKI (odds ratio [OR], 2.55 [1.36-4.78] per log copy/uL; = 0.003). Patients with AKI had higher nucleosome levels at presentation (β = 0.32 [0.00-0.63] arbitrary unit; = 0.048), a difference that was more pronounced at 24 hours (β = 0.41 [0.06-0.76]; = 0.021) and 48 hours (β = 0.71 [0.35-1.08]; < 0.001) ( = 0.075, interaction with time point).
Plasma nucleic acid DAMPs have distinct kinetics and associations with AKI in critically ill trauma patients. nDNA at presentation predicts subsequent AKI and may be amenable to targeted therapies in this population.
循环核酸,单独存在以及与组蛋白结合形成核小体的形式,已被认为是创伤后全身炎症和凝血与急性肾损伤(AKI)之间的联系。我们试图确定创伤后多个时间点测量的循环核酸与AKI风险之间的关联。
我们对创伤患者进行了一项前瞻性队列研究,在患者就诊时、6小时、12小时、24小时和48小时采集血浆,根据改善全球肾脏病预后组织(KDIGO)的血清肌酐和透析标准在最初6天内定义AKI。我们使用多变量线性混合效应模型确定各时间点血浆线粒体DNA(mtDNA)、核DNA(nDNA)和核小体水平的动力学以及与AKI的关联,并对损伤特征和输血情况进行了调整。我们使用多变量逻辑回归评估就诊时核酸损伤相关分子模式(DAMP)浓度与随后发生的AKI之间的关联,并对损伤严重程度进行了调整。
一级学术创伤中心。
创伤患者(n = 55),就诊后需要重症监护≥24小时。
无。
17例患者(31%)发生AKI,中位时间为就诊后12.0小时(四分位间距,6.2 - 24.1小时)。mtDNA与AKI呈随时间变化的关联(P = 0.