Department of Pathology, Brigham and Women's Hospital, Boston, Massachusetts.
Harvard Medical School, Boston, Massachusetts.
Kidney360. 2021 Jul 14;2(10):1560-1568. doi: 10.34067/KID.0003312021. eCollection 2021 Oct 28.
AKI is an abrupt decrease in kidney function associated with significant morbidity and mortality. Electronic notifications of AKI have been utilized in patients who are hospitalized, but their efficacy in the outpatient setting is unclear.
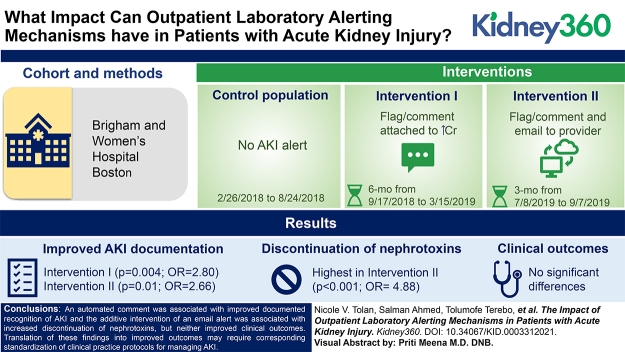
We evaluated the effect of two outpatient interventions: an automated comment on increasing creatinine results (intervention I; 6 months; =159) along with an email to the provider (intervention II; 3 months; =105), compared with a control (baseline; 6 months; =176). A comment was generated if a patient's creatinine increased by >0.5 mg/dl (previous creatinine ≤2.0 mg/dl) or by 50% (previous creatinine >2.0 mg/dl) within 180 days. Process measures included documentation of AKI and clinical actions. Clinical outcomes were defined as recovery from AKI within 7 days, prolonged AKI from 8 to 89 days, and progression to CKD with in 120 days.
Providers were more likely to document AKI in interventions I (=0.004; OR, 2.80; 95% CI, 1.38 to 5.67) and II (=0.01; OR, 2.66; 95% CI, 1.21 to 5.81). Providers were also more likely to discontinue nephrotoxins in intervention II (<0.001; OR, 4.88; 95% CI, 2.27 to 10.50). The median time to follow-up creatinine trended shorter among patients with AKI documented (21 versus 42 days; =0.11). There were no significant differences in clinical outcomes.
An automated comment was associated with improved documented recognition of AKI and the additive intervention of an email alert was associated with increased discontinuation of nephrotoxins, but neither improved clinical outcomes. Translation of these findings into improved outcomes may require corresponding standardization of clinical practice protocols for managing AKI.
急性肾损伤(AKI)是一种肾功能急剧下降的疾病,与较高的发病率和死亡率相关。电子通知系统已在住院患者中用于 AKI,但在门诊环境下的效果尚不清楚。
我们评估了两种门诊干预措施的效果:对肌酐升高结果(干预 I;6 个月;=159)自动生成评论,以及向医务人员发送电子邮件(干预 II;3 个月;=105),与对照组(基线;6 个月;=176)进行比较。如果患者的肌酐在 180 天内升高超过 0.5mg/dl(上次肌酐≤2.0mg/dl)或增加 50%(上次肌酐>2.0mg/dl),则生成评论。过程测量包括 AKI 的记录和临床措施。临床结局定义为 7 天内 AKI 恢复、8 至 89 天内 AKI 延长和 120 天内进展为慢性肾脏病(CKD)。
干预 I(=0.004;比值比,2.80;95%置信区间,1.38 至 5.67)和 II(=0.01;比值比,2.66;95%置信区间,1.21 至 5.81)中,医务人员更有可能记录 AKI。在干预 II 中,医务人员更有可能停止使用肾毒性药物(<0.001;比值比,4.88;95%置信区间,2.27 至 10.50)。记录 AKI 的患者的中位随访肌酐时间更短(21 天与 42 天;=0.11)。两组间临床结局无显著差异。
自动评论与 AKI 诊断记录的改善有关,而电子邮件提醒的附加干预与肾毒性药物的停用增加有关,但两者均未改善临床结局。要将这些发现转化为改善结局,可能需要对 AKI 管理的临床实践方案进行相应的标准化。