Division of Nephrology, Department of Medicine, University of California San Diego, San Diego, California, United States of America.
College of Medicine, University of Malawi, Blantyre, Malawi.
PLoS Med. 2021 Jan 14;18(1):e1003408. doi: 10.1371/journal.pmed.1003408. eCollection 2021 Jan.
Acute kidney injury (AKI) is increasingly encountered in community settings and contributes to morbidity, mortality, and increased resource utilization worldwide. In low-resource settings, lack of awareness of and limited access to diagnostic and therapeutic interventions likely influence patient management. We evaluated the feasibility of the use of point-of-care (POC) serum creatinine and urine dipstick testing with an education and training program to optimize the identification and management of AKI in the community in 3 low-resource countries.
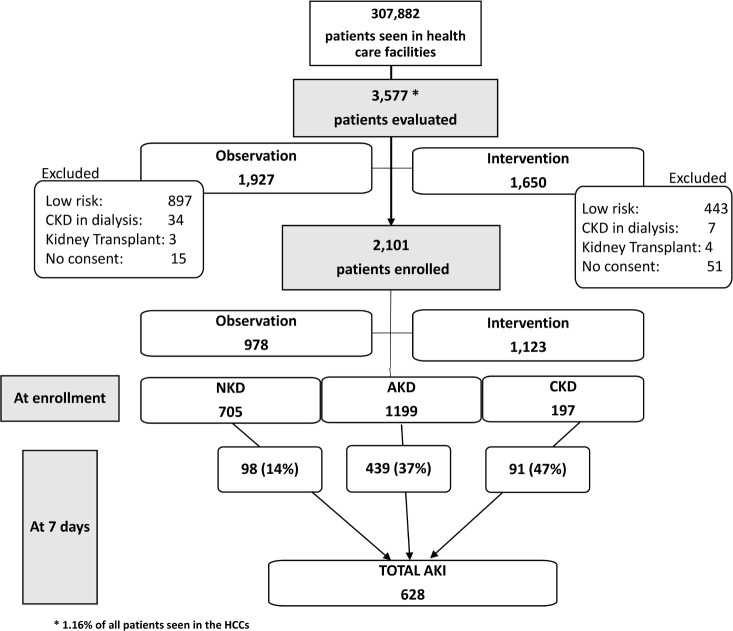
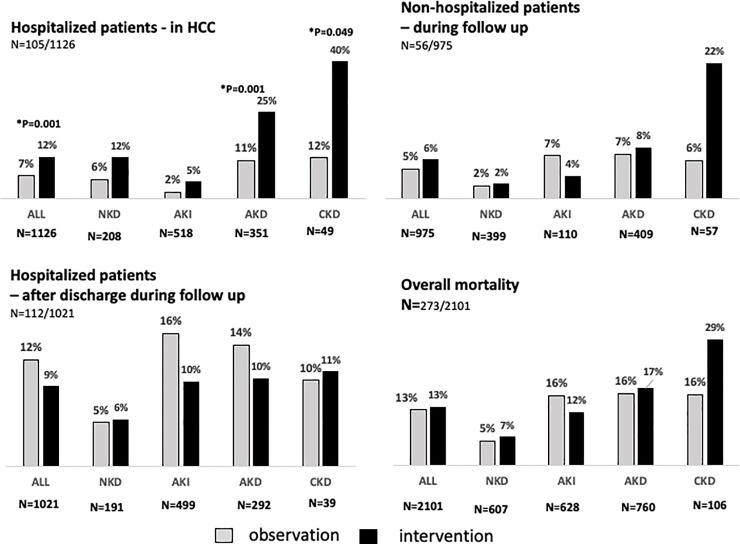
Patients presenting to healthcare centers (HCCs) from 1 October 2016 to 29 September 2017 in the cities Cochabamba, Bolivia; Dharan, Nepal; and Blantyre, Malawi, were assessed utilizing a symptom-based risk score to identify patients at moderate to high AKI risk. POC testing for serum creatinine and urine dipstick at enrollment were utilized to classify these patients as having chronic kidney disease (CKD), acute kidney disease (AKD), or no kidney disease (NKD). Patients were followed for a maximum of 6 months with repeat POC testing. AKI development was assessed at 7 days, kidney recovery at 1 month, and progression to CKD and mortality at 3 and 6 months. Following an observation phase to establish baseline data, care providers and physicians in the HCCs were trained with a standardized protocol utilizing POC tests to evaluate and manage patients, guided by physicians in referral hospitals connected via mobile digital technology. We evaluated 3,577 patients, and 2,101 were enrolled: 978 in the observation phase and 1,123 in the intervention phase. Due to the high number of patients attending the centers daily, it was not feasible to screen all patients to assess the actual incidence of AKI. Of enrolled patients, 1,825/2,101 (87%) were adults, 1,117/2,101 (53%) were females, 399/2,101 (19%) were from Bolivia, 813/2,101 (39%) were from Malawi, and 889/2,101 (42%) were from Nepal. The age of enrolled patients ranged from 1 month to 96 years, with a mean of 43 years (SD 21) and a median of 43 years (IQR 27-62). Hypertension was the most common comorbidity (418/2,101; 20%). At enrollment, 197/2,101 (9.4%) had CKD, and 1,199/2,101 (57%) had AKD. AKI developed in 30% within 7 days. By 1 month, 268/978 (27%) patients in the observation phase and 203/1,123 (18%) in the intervention phase were lost to follow-up. In the intervention phase, more patients received fluids (observation 714/978 [73%] versus intervention 874/1,123 [78%]; 95% CI 0.63, 0.94; p = 0.012), hospitalization was reduced (observation 578/978 [59%] versus intervention 548/1,123 [49%]; 95% CI 0.55, 0.79; p < 0.001), and admitted patients with severe AKI did not show a significantly lower mortality during follow-up (observation 27/135 [20%] versus intervention 21/178 [11.8%]; 95% CI 0.98, 3.52; p = 0.057). Of 504 patients with kidney function assessed during the 6-month follow-up, de novo CKD arose in 79/484 (16.3%), with no difference between the observation and intervention phase (95% CI 0.91, 2.47; p = 0.101). Overall mortality was 273/2,101 (13%) and was highest in those who had CKD (24/106; 23%), followed by those with AKD (128/760; 17%), AKI (85/628; 14%), and NKD (36/607; 6%). The main limitation of our study was the inability to determine the actual incidence of kidney dysfunction in the health centers as it was not feasible to screen all the patients due to the high numbers seen daily.
This multicenter, non-randomized feasibility study in low-resource settings demonstrates that it is feasible to implement a comprehensive program utilizing POC testing and protocol-based management to improve the recognition and management of AKI and AKD in high-risk patients in primary care.
急性肾损伤(AKI)在社区环境中越来越常见,导致发病率、死亡率和全球资源利用率增加。在资源匮乏的环境中,对诊断和治疗干预措施的认识不足以及获取途径有限,可能影响患者的管理。我们评估了在 3 个资源匮乏国家中使用即时检测(POC)血清肌酐和尿液试纸检测并结合教育和培训计划来优化社区中 AKI 的识别和管理的可行性。
2016 年 10 月 1 日至 2017 年 9 月 29 日期间,在玻利维亚科恰班巴市、尼泊尔的达兰市和马拉维的布兰太尔市的医疗中心就诊的患者利用基于症状的风险评分来识别具有中高度 AKI 风险的患者。在入组时利用 POC 检测血清肌酐和尿液试纸来分类这些患者患有慢性肾脏病(CKD)、急性肾损伤(AKD)或无肾脏病(NKD)。患者接受了最长 6 个月的随访,并重复进行 POC 检测。在第 7 天评估 AKI 进展,第 1 个月评估肾功能恢复,第 3 和 6 个月评估进展为 CKD 和死亡率。在观察阶段建立基线数据后,医疗中心的医护人员接受了利用 POC 检测评估和管理患者的标准化培训,通过与通过移动数字技术连接的转诊医院的医生进行指导。我们评估了 3577 名患者,其中 2101 名入组:978 名在观察阶段,1123 名在干预阶段。由于每天有大量患者就诊,不可能对所有患者进行筛查以评估 AKI 的实际发病率。在入组的患者中,1825/2101(87%)为成年人,1117/2101(53%)为女性,399/2101(19%)来自玻利维亚,813/2101(39%)来自马拉维,889/2101(42%)来自尼泊尔。入组患者的年龄范围为 1 个月至 96 岁,平均年龄为 43 岁(SD 21),中位数为 43 岁(IQR 27-62)。高血压是最常见的合并症(418/2101;20%)。入组时,197/2101(9.4%)患有 CKD,1199/2101(57%)患有 AKD。30%的患者在 7 天内发生 AKI。在观察阶段,268/978(27%)名患者和干预阶段 203/1123(18%)名患者在 1 个月时失访。在干预阶段,更多的患者接受了液体治疗(观察 714/978 [73%] 与干预 874/1123 [78%];95%CI 0.63,0.94;p = 0.012),住院率降低(观察 578/978 [59%] 与干预 548/1123 [49%];95%CI 0.55,0.79;p < 0.001),并且在随访期间,患有严重 AKI 的住院患者死亡率没有显著降低(观察 27/135 [20%] 与干预 21/178 [11.8%];95%CI 0.98,3.52;p = 0.057)。在 6 个月的随访期间,对 504 名患者的肾功能进行了评估,新出现 CKD 79/484(16.3%),观察组和干预组之间无差异(95%CI 0.91,2.47;p = 0.101)。总的死亡率为 273/2101(13%),其中 CKD 患者的死亡率最高(24/106;23%),其次是 AKD 患者(128/760;17%)、AKI 患者(85/628;14%)和 NKD 患者(36/607;6%)。我们研究的主要限制是由于每天就诊的患者人数众多,因此无法确定医疗中心中肾功能障碍的实际发病率,因此无法对所有患者进行筛查。
这项在资源匮乏环境中进行的多中心、非随机可行性研究表明,利用 POC 检测和基于方案的管理实施综合计划,以提高初级保健中高危患者 AKI 和 AKD 的识别和管理是可行的。