Department of Surgery, The Lambe Institute for Translational Research, National University of Ireland, Galway, Ireland.
BJS Open. 2022 Mar 8;6(2). doi: 10.1093/bjsopen/zrac022.
Axillary lymph node status remains the most powerful prognostic indicator in invasive breast cancer. Ductal carcinoma in situ (DCIS) is a non-invasive disease and does not spread to axillary lymph nodes. The presence of an invasive component to DCIS mandates nodal evaluation through sentinel lymph node biopsy (SLNB). Quantification of the necessity of upfront SLNB for DCIS requires investigation. The aim was to establish the likelihood of having a positive SLNB (SLNB+) for DCIS and to establish parameters predictive of SLNB+.
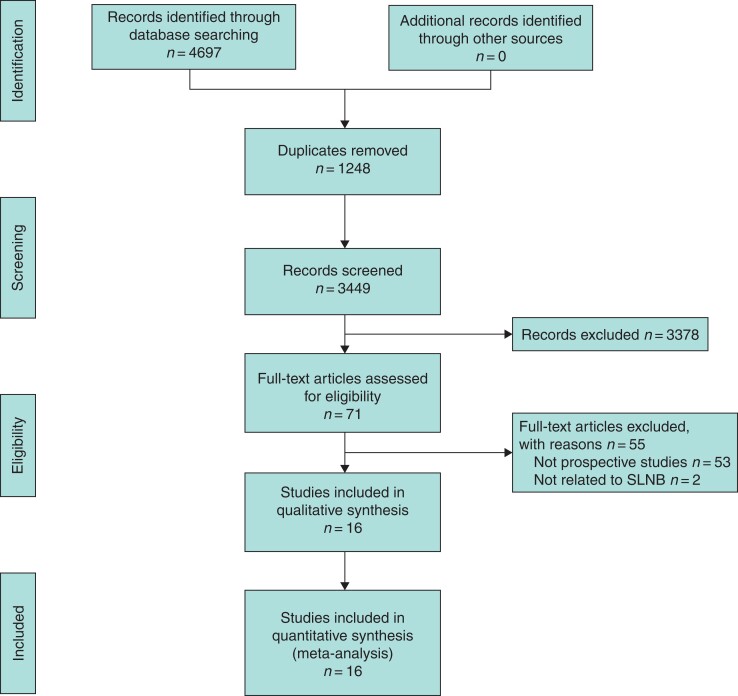
A systematic review was performed as per the PRISMA guidelines. Prospective studies only were included. Characteristics predictive of SLNB+ were expressed as dichotomous variables and pooled as odds ratios (o.r.) and associated 95 per cent confidence intervals (c.i.) using the Mantel-Haenszel method.
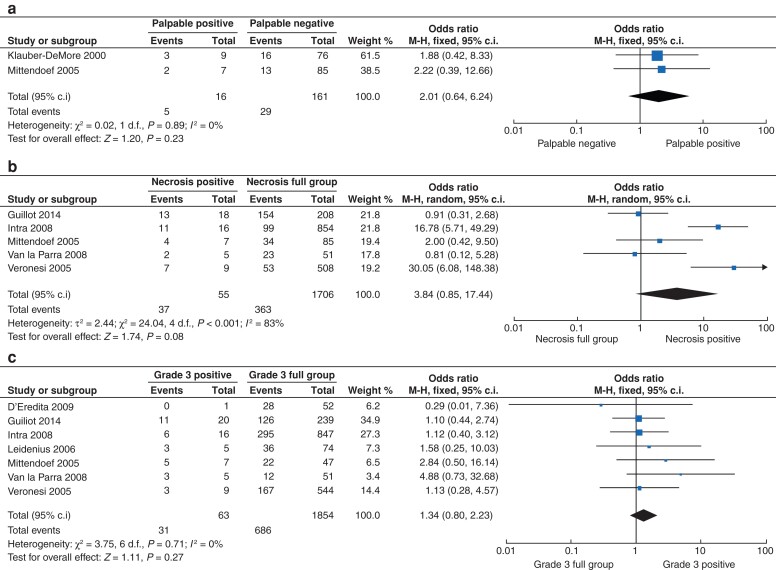
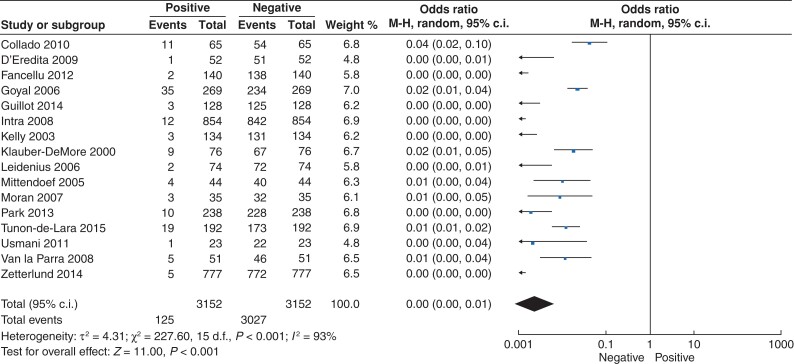
Overall, 16 studies including 4388 patients were included (mean patient age 54.8 (range 24 to 92) years). Of these, 72.5 per cent of patients underwent SLNB (3156 of 4356 patients) and 4.9 per cent had SLNB+ (153 of 3153 patients). The likelihood of having SLNB+ for DCIS was less than 1 per cent (o.r. <0.01, 95 per cent c.i. 0.00 to 0.01; P < 0.001, I2 = 93 per cent). Palpable DCIS (o.r. 2.01, 95 per cent c.i. 0.64 to 6.24; P = 0.230, I2 = 0 per cent), tumour necrosis (o.r. 3.84, 95 per cent c.i. 0.85 to 17.44; P = 0.080, I2 = 83 per cent), and grade 3 DCIS (o.r. 1.34, 95 per cent c.i. 0.80 to 2.23; P = 0.270, I2 = 0 per cent) all trended towards significance in predicting SLNB+.
While aggressive clinicopathological parameters may guide SLNB for patients with DCIS, the absolute and relative risk of SLNB+ for DCIS is less than 5 per cent and 1 per cent, respectively. Well-designed randomized controlled trials are required to establish fully the necessity of SLNB for patients diagnosed with DCIS.
CRD42021284194 (https://www.crd.york.ac.uk/prospero/).
腋窝淋巴结状态仍然是浸润性乳腺癌最有力的预后指标。导管原位癌(DCIS)是一种非浸润性疾病,不会扩散到腋窝淋巴结。DCIS 存在浸润性成分,需要通过前哨淋巴结活检(SLNB)进行淋巴结评估。需要研究明确 DCIS 行 SLNB 的必要性。目的是确定 DCIS 行 SLNB 的阳性预测值(SLNB+)的可能性,并确定预测 SLNB+的参数。
按照 PRISMA 指南进行系统评价。仅纳入前瞻性研究。以二项变量的形式表达预测 SLNB+的特征,并使用 Mantel-Haenszel 法汇总为比值比(o.r.)和相关 95%置信区间(c.i.)。
共纳入 16 项研究,包括 4388 例患者(平均患者年龄 54.8 岁[范围 24 至 92 岁])。其中,72.5%的患者行 SLNB(3156 例患者中的 3156 例),4.9%的患者 SLNB+(3153 例患者中的 153 例)。DCIS 行 SLNB+的可能性小于 1%(o.r. <0.01,95%c.i. 0.00 至 0.01;P<0.001,I2=93%)。可触及的 DCIS(o.r. 2.01,95%c.i. 0.64 至 6.24;P=0.230,I2=0%)、肿瘤坏死(o.r. 3.84,95%c.i. 0.85 至 17.44;P=0.080,I2=83%)和 3 级 DCIS(o.r. 1.34,95%c.i. 0.80 至 2.23;P=0.270,I2=0%)均提示预测 SLNB+有趋势。
虽然侵袭性临床病理参数可能指导 DCIS 患者的 SLNB,但 DCIS 行 SLNB+的绝对和相对风险分别小于 5%和 1%。需要设计良好的随机对照试验来充分确定诊断为 DCIS 的患者行 SLNB 的必要性。
CRD42021284194(https://www.crd.york.ac.uk/prospero/)。