Department of Medical Oncology, Kochi Medical School, Kochi, Japan.
Department of Gastroenterological Surgery, Osaka General Medical Center, Osaka, Japan.
Adv Ther. 2022 Jun;39(6):2596-2613. doi: 10.1007/s12325-022-02122-4. Epub 2022 Apr 6.
Evidence is lacking on second-line and later treatments for patients with RAS wild-type colorectal cancer (CRC) who receive first-line anti-epidermal growth factor receptor (EGFR) antibody therapy. In this study, we explored the real-world treatment sequences, treatment duration, and factors associated with treatment sequences and durations in Japanese patients with CRC.
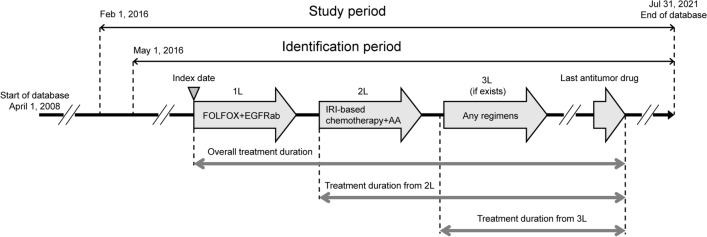
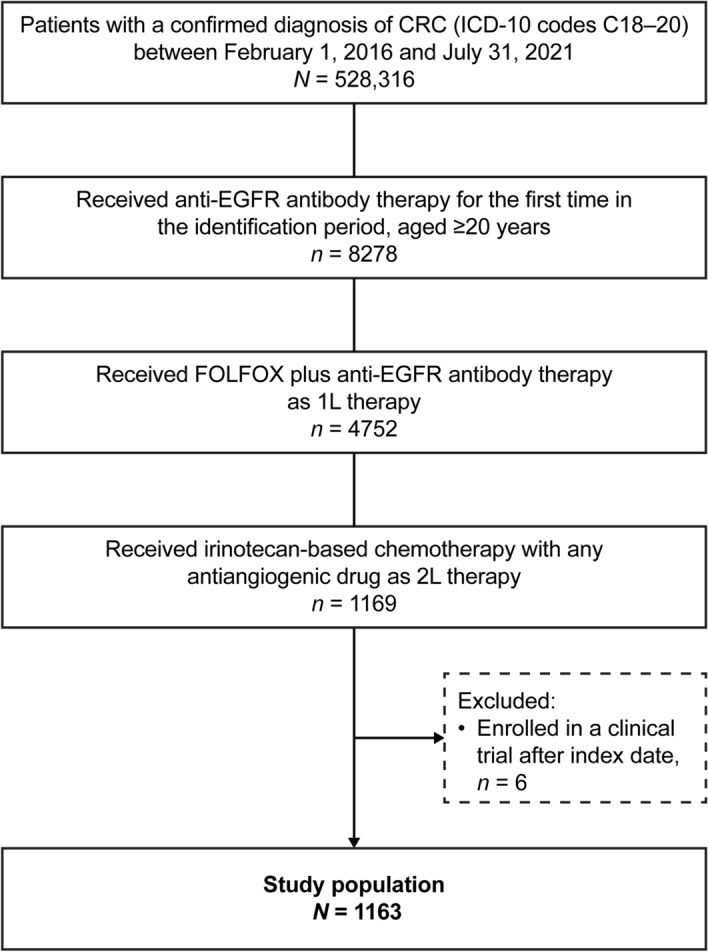
This retrospective observational cohort study used a Japanese administrative claims database (April 2008 to July 2021). Patients with confirmed CRC (presumed RAS wild-type) who received first-line FOLFOX (leucovorin + 5-fluorouracil + oxaliplatin) plus anti-EGFR therapy in or after May 2016, followed by second-line irinotecan-based chemotherapy plus an antiangiogenic drug, were included. Treatment durations were estimated by the Kaplan-Meier method. Cox regression analysis was used to identify factors associated with treatment duration.
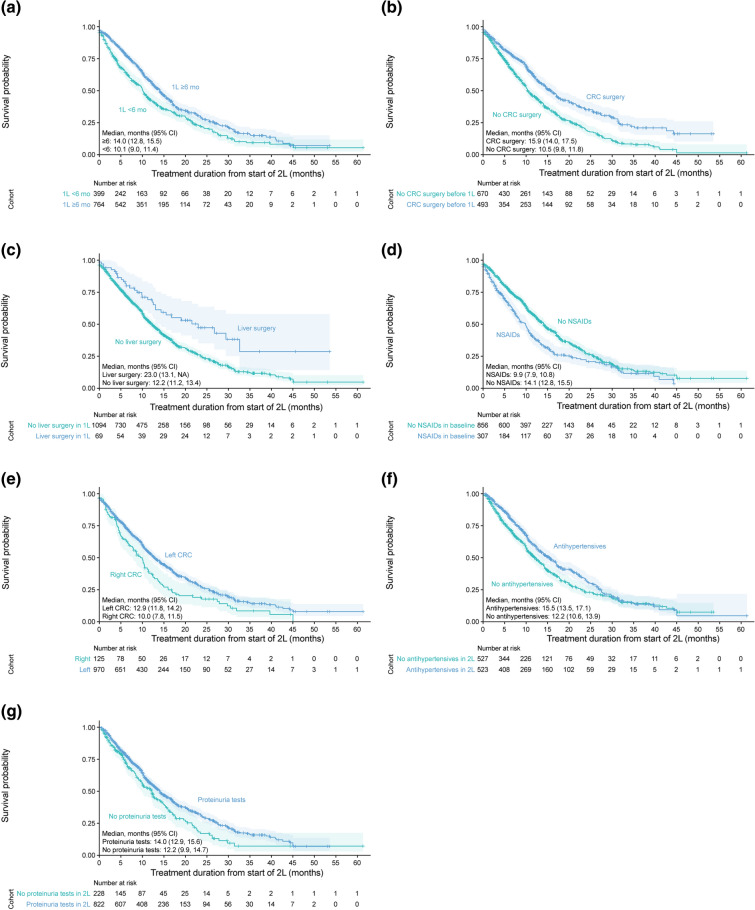
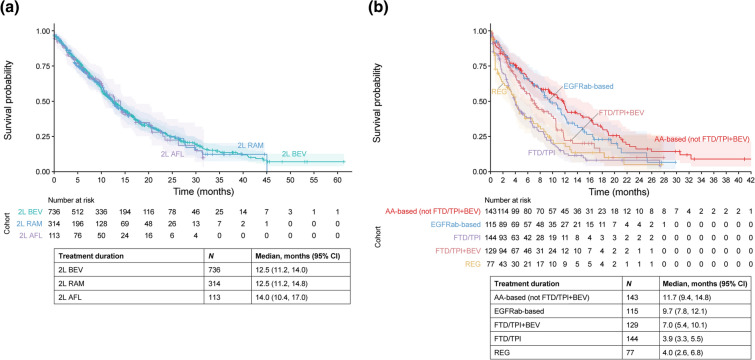
Analysis populations consisted of 1163 (first-line and second-line) and 645 (third-line) patients. At the start of first-line therapy, 67.8% of patients were male, the mean age was 64 years, 83.4% had left-sided CRC, and 84.3% were prescribed FOLFOX plus panitumumab. For second-line therapy, patients were prescribed bevacizumab (63%), ramucirumab (27%), or aflibercept beta (10%). Median (95% CI) treatment durations from the start of second-line therapy to the end of antitumor drug therapies were similar for bevacizumab (12.5 months [11.2, 14.0]), ramucirumab (12.5 months [11.2, 14.8]), and aflibercept beta (14.0 months [10.4, 17.0]). Treatment duration from second-line was positively associated with first-line treatment duration of 6 months or more, CRC surgery before starting first-line therapy, and liver surgery during first-line therapy, and was negatively associated with use of nonsteroidal anti-inflammatory drugs before second-line therapy.
Real-world data revealed that all three antiangiogenic drugs were used as second-line therapy after first-line anti-EGFR antibodies and showed similar treatment durations.
对于接受一线抗表皮生长因子受体(EGFR)抗体治疗后 RAS 野生型结直肠癌(CRC)患者的二线及后续治疗,目前缺乏相关证据。在这项研究中,我们探索了日本 CRC 患者的真实世界治疗方案、治疗持续时间以及与治疗方案和持续时间相关的因素。
本回顾性观察性队列研究使用了日本行政索赔数据库(2008 年 4 月至 2021 年 7 月)。符合以下条件的患者被纳入研究:确诊为 CRC(假定 RAS 野生型),于 2016 年 5 月后接受一线 FOLFOX(亚叶酸钙+5-氟尿嘧啶+奥沙利铂)加抗 EGFR 治疗,随后接受二线伊立替康为基础的化疗加抗血管生成药物治疗。采用 Kaplan-Meier 法估计治疗持续时间。采用 Cox 回归分析确定与治疗持续时间相关的因素。
分析人群包括 1163 例(一线和二线)和 645 例(三线)患者。在一线治疗开始时,67.8%的患者为男性,平均年龄为 64 岁,83.4%为左侧 CRC,84.3%的患者处方为 FOLFOX 加帕尼单抗。二线治疗时,患者处方贝伐珠单抗(63%)、雷莫芦单抗(27%)或阿柏西普β(10%)。从二线治疗开始到抗肿瘤药物治疗结束的二线治疗中位(95%CI)持续时间,贝伐珠单抗为 12.5 个月(11.2,14.0),雷莫芦单抗为 12.5 个月(11.2,14.8),阿柏西普β为 14.0 个月(10.4,17.0)。二线治疗的持续时间与一线治疗持续时间为 6 个月或更长、一线治疗前接受 CRC 手术以及一线治疗期间接受肝脏手术呈正相关,与二线治疗前使用非甾体抗炎药呈负相关。
真实世界数据显示,一线抗 EGFR 抗体治疗后,所有三种抗血管生成药物均被用作二线治疗,且治疗持续时间相似。