Universidade da Região de Joinville, Programa de Pós-Graduação em Saúde e Meio Ambiente, Joinville, SC, Brasil.
Fundação Pró-Rim, Joinville, SC, Brasil.
J Bras Nefrol. 2022 Oct-Dec;44(4):482-489. doi: 10.1590/2175-8239-JBN-2021-0182.
Urgent-start peritoneal dialysis (US-PD) has been proposed as a safe modality of renal replacement therapy (RRT) for end-stage renal disease (ESRD) patients with an indication for emergency dialysis initiation. We aimed to compare the characteristics, 30-day complications, and clinical outcomes of US-PD and planned peritoneal dialysis (Plan-PD) patients over the first year of therapy.
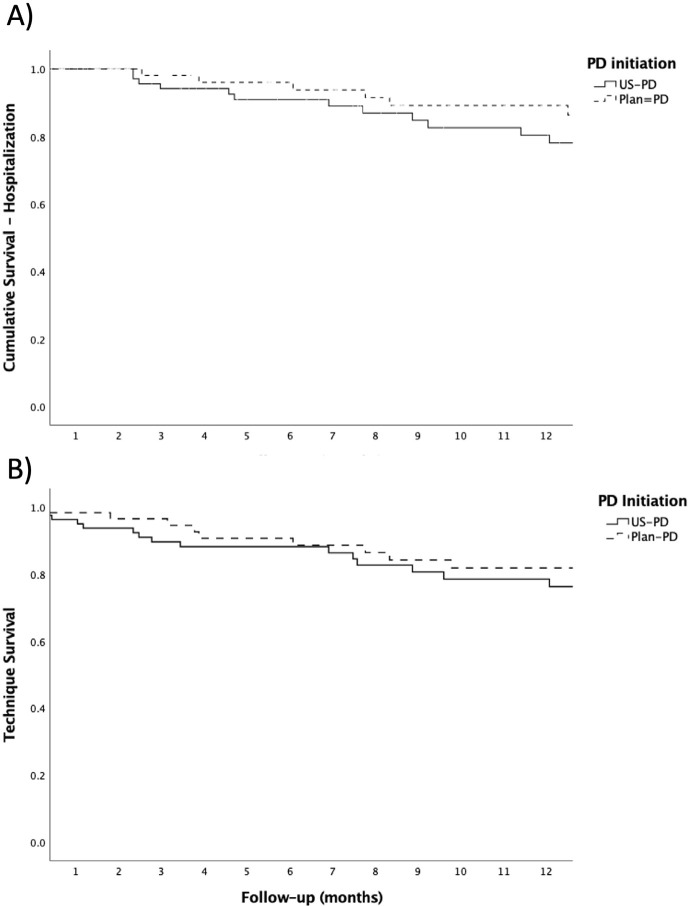
This was a single-center retrospective study that included incident adult patients followed for up to one year. US-PD was considered when incident patients started therapy within 7 days after Tenckhoff catheter implantation. Plan-PD group consisted of patients who started therapy after the breaking period (15 days). Mechanical and infectious complications were compared 30 days from PD initiation. Hospitalization and technique failure during the first 12 months on PD were assessed by Kaplan-Meier curves and the determinants were calculated by Cox regression models.
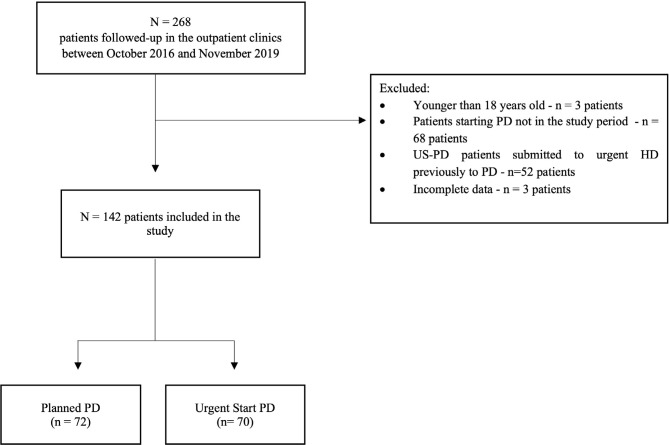
All patients starting PD between October/2016 and November/2019 who fulfilled the inclusion criteria were analyzed. We evaluated 137 patients (70 in the US-PD x 67 Plan-PD). The main complications in the first 30 days were catheter tip migration (7.5% Plan-PD x 4.3% US-PD - p= 0.49) and leakage (4.5% Plan-PD x 5.7% US-PD - p=0.74). Most catheters were placed using the Seldinger technique. The main cause of dropout was death in US-PD patients (15.7%) and transfer to HD in Plan-PD patients (13.4%). The occurrence of complications in the first 30 days was the only risk factor for dropout (OR = 2.9; 95% CI 1.1-7.5, p = 0.03). Hospitalization rates and technique survival were similar in both groups.
The lack of significant differences in patients' outcomes between groups reinforces that PD is a safe and applicable dialysis method in patients who need immediate dialysis.
紧急启动腹膜透析(US-PD)已被提议作为一种安全的肾脏替代治疗(RRT)方式,适用于需要紧急透析启动的终末期肾病(ESRD)患者。我们旨在比较 US-PD 和计划腹膜透析(Plan-PD)患者在治疗的第一年中的特征、30 天并发症和临床结局。
这是一项单中心回顾性研究,纳入了接受治疗的成年患者,随访时间最长为一年。当患者在 Tenckhoff 导管植入后 7 天内开始治疗时,被认为是 US-PD。Plan-PD 组由在突破期(15 天)后开始治疗的患者组成。比较 PD 开始后 30 天的机械和感染并发症。通过 Kaplan-Meier 曲线评估第一个 12 个月 PD 期间的住院和技术失败情况,并通过 Cox 回归模型计算决定因素。
所有符合纳入标准的 2016 年 10 月至 2019 年 11 月期间开始 PD 的患者均进行了分析。我们评估了 137 名患者(70 名 US-PD 组和 67 名 Plan-PD 组)。前 30 天的主要并发症是导管尖端迁移(4.5% Plan-PD 组和 5.7% US-PD 组,p=0.74)和渗漏(4.5% Plan-PD 组和 5.7% US-PD 组,p=0.49)。大多数导管均采用 Seldinger 技术放置。US-PD 患者的主要退出原因是死亡(15.7%),Plan-PD 患者的主要退出原因是转至血液透析(HD)(13.4%)。前 30 天并发症的发生是退出的唯一危险因素(OR=2.9;95%CI 1.1-7.5,p=0.03)。两组的住院率和技术生存率相似。
两组患者结局无显著差异,这进一步证实 PD 是一种安全且适用的透析方法,适用于需要立即透析的患者。