Department of Gastroenterology, Royal Liverpool Hospital, Liverpool University Hospitals NHS Foundation Trust, Liverpool, UK.
Department of Gastroenterology, Aintree University Hospital, Liverpool University Hospitals NHS Foundation Trust, Liverpool, UK.
J Crohns Colitis. 2022 Sep 8;16(9):1436-1446. doi: 10.1093/ecco-jcc/jjac053.
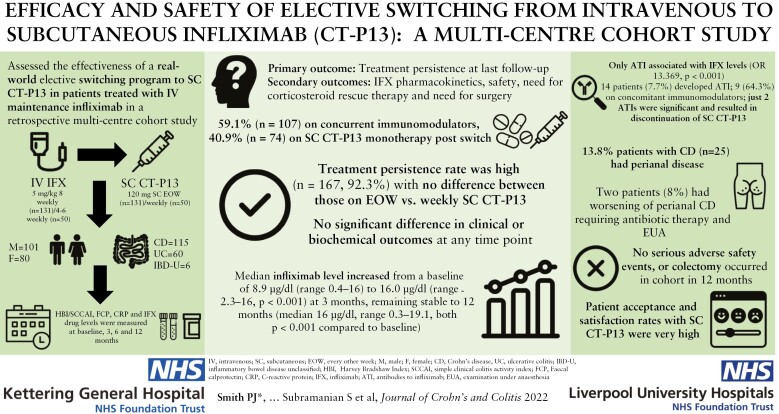
Intravenous [IV] infliximab is a well-established therapy for inflammatory bowel diseases [IBD] patients. A subcutaneous [SC] formulation of infliximab [CT-P13] has recently been shown to be as effective as IV infliximab after two doses of IV induction in a randomised trial, but there are no data to support elective switching of patients on maintenance IV infliximab therapy. We aimed to assess the effectiveness of an elective switching programme to SC CT-P13 in patients treated with IV infliximab.
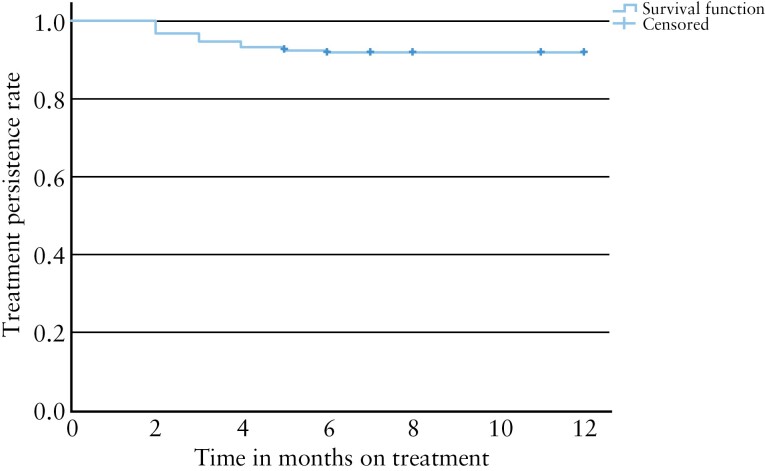
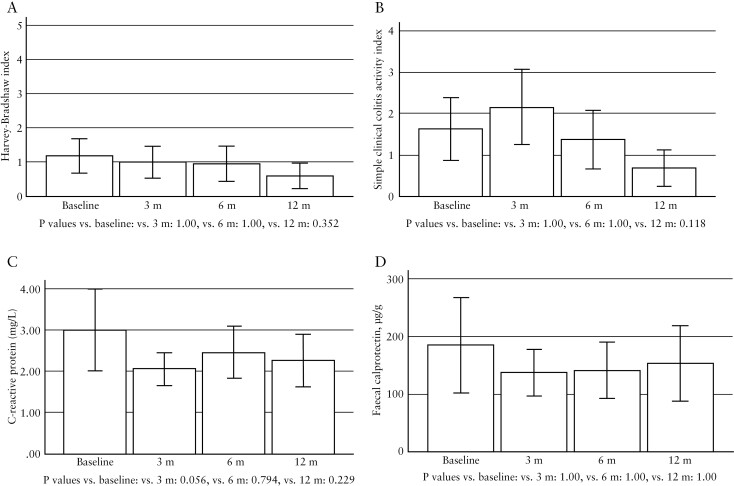
Patients on established maintenance IV infliximab, who switched to SC CT-P13, were included in this retrospective multicentre cohort study. Disease activity was monitored serially with the Harvey-Bradshaw Index [HBI] for Crohn's disease [CD] and the Simple Clinical Colitis Activity Index [SCCAI] for ulcerative colitis (UC) for up to 12 months at months 3, 6, and 12. Faecal calprotectin [FC] and C-reactive protein [CRP] were recorded at baseline and follow-up, if available. Infliximab trough levels were measured prior to switch and at months 3, 6, and 12 following switch. The primary outcome measure was treatment persistence at latest follow-up. Secondary outcome measures included infliximab pharmacokinetics [PK], safety, need for corticosteroid rescue therapy, and need for surgery.
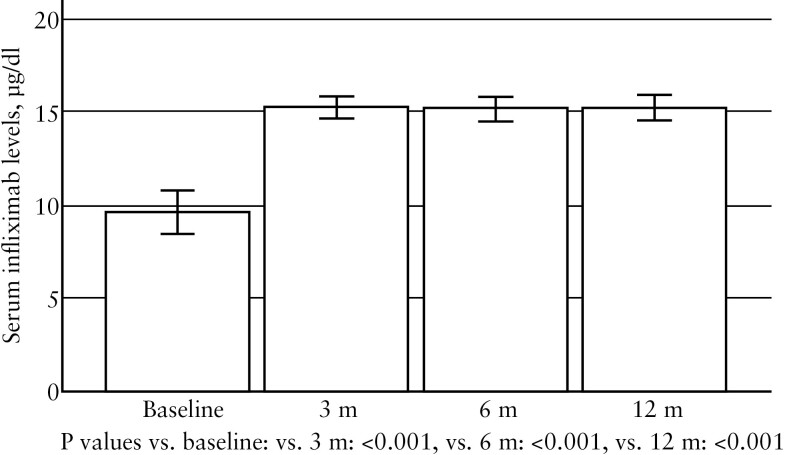
We included 181 patients, of whom 115 [63.5%] had CD. The majority [72.4%] were on 8-weekly dosing of intravenous infliximab prior to switching, and more than half [59.1%] were on concomitant immunomodulatory therapy. The majority of patients (CD: 106, 92.2%; UC: 46, 76.7%; and IBD unclassified [IBD-U]: 5, 83.3%) were in clinical remission. Treatment persistence rate was high [n = 167, 92.3%] and only 14 patients [7.7%] stopped treatment during the follow-up period. There was no significant difference between baseline and repeat measurements at 3, 6, or 12 months for HBI, SCCAI, CRP, or FC. Of the total cohort, 25 patients (13.8%) had perianal CD. Of these, only two patients [8%] had worsening of perianal CD and required antibiotic therapy and further examination under anaesthesia [EUA]. Both these patients also switched back to intravenous infliximab. Median infliximab level increased from a baseline of 8.9 µg/dl [range 0.4-16] to 16.0 µg/dl [range 2.3-16, p <0.001] at 3 months. Serum levels stayed stable at 6 months [median 16 µg/dl, range 0.3-17.2] and 12 months [median 16 µg/dl, range 0.3-19.1, both p <0.001 compared with baseline]. Among the variables examined, only antibodies to infliximab [ATI] was associated with infliximab levels (odds ratio [OR] -13.369, 95% CI -15.405, -11.333, p <0.001]. A total of 14 patients [7.7%] developed ATI; of these, nine [64.3%] were on concomitant immunomodulatory therapy. Immunomodulatory therapy was not significantly associated with development of ATI [p = 0.15]. In a subset of patients receiving escalated IV infliximab dosing frequency prior to switching, no difference in treatment persistence was observed in patients receiving weekly versus alternate weekly SC CT-P13. Patient acceptance and satisfaction rates with SC CT-P13 were very high.
Among patients on IV infliximab maintenance therapy switched to SC CT-P13, we observed high treatment persistence rates and low rates of immunogenicity, with no change in clinical disease activity indices or biomarkers. Infliximab levels increased after switch to SC CT-P13, and only ATI was associated with serum infliximab levels. Patient acceptance and satisfaction rates were high with SC CT-P13.
静脉内(IV)英夫利昔单抗是炎症性肠病(IBD)患者的一种成熟的治疗方法。最近的一项随机试验表明,皮下(SC)英夫利昔单抗[CT-P13]制剂在接受两剂 IV 诱导后与 IV 英夫利昔单抗同样有效,但尚无数据支持对维持 IV 英夫利昔单抗治疗的患者进行选择性转换。我们旨在评估在接受 IV 英夫利昔单抗治疗的患者中进行选择性转换计划到 SC CT-P13 的疗效。
纳入了接受 IV 英夫利昔单抗维持治疗并转换为 SC CT-P13 的患者,进行了这项回顾性多中心队列研究。在第 3、6 和 12 个月时,使用 Harvey-Bradshaw 指数(HBI)评估克罗恩病(CD)的疾病活动度,使用简单临床结肠炎活动指数(SCCAI)评估溃疡性结肠炎(UC)的疾病活动度。如果有条件,在基线和随访时记录粪便钙卫蛋白(FC)和 C 反应蛋白(CRP)。在转换前和转换后第 3、6 和 12 个月时测量英夫利昔单抗谷水平。主要终点是随访时的治疗持续性。次要终点包括英夫利昔单抗药代动力学(PK)、安全性、皮质类固醇解救治疗的需要和手术的需要。
我们纳入了 181 例患者,其中 115 例(63.5%)患有 CD。大多数患者(72.4%)在转换前接受了 8 周的 IV 英夫利昔单抗治疗,超过一半(59.1%)接受了免疫调节剂联合治疗。大多数患者(CD:106 例,92.2%;UC:46 例,76.7%;和 IBD 未分类[IBD-U]:5 例,83.3%)处于临床缓解状态。治疗持续性率很高[n=167,92.3%],只有 14 例患者(7.7%)在随访期间停止治疗。在 3、6 或 12 个月时,HBI、SCCAI、CRP 或 FC 无显著差异。在总队列中,25 例(13.8%)患者患有肛周 CD。其中,只有 2 例患者(8%)肛周 CD 恶化,需要抗生素治疗和进一步麻醉下检查[EUA]。这两名患者也转回了静脉内英夫利昔单抗治疗。英夫利昔单抗水平中位数从基线的 8.9µg/dl[范围 0.4-16]增加到 3 个月时的 16µg/dl[范围 2.3-16,p<0.001]。6 个月时血清水平稳定[中位数 16µg/dl,范围 0.3-17.2],12 个月时稳定[中位数 16µg/dl,范围 0.3-19.1,均与基线相比 p<0.001]。在检查的变量中,只有英夫利昔单抗抗体[ATI]与英夫利昔单抗水平相关(比值比[OR] -13.369,95%CI -15.405,-11.333,p<0.001)。共有 14 例患者(7.7%)出现 ATI;其中 9 例(64.3%)接受了免疫调节剂联合治疗。免疫调节剂的使用与 ATI 的发生无显著相关性(p=0.15)。在接受转换前增加 IV 英夫利昔单抗给药频率的患者亚组中,每周与交替每周接受 SC CT-P13 的患者在治疗持续性方面无差异。
在接受 IV 英夫利昔单抗维持治疗的患者中,转换为 SC CT-P13 后,我们观察到高治疗持续性率和低免疫原性率,临床疾病活动指数或生物标志物无变化。转换后英夫利昔单抗水平增加,只有 ATI 与血清英夫利昔单抗水平相关。患者对 SC CT-P13 的接受度和满意度非常高。