Argüelles-Arias Federico, Guerra Veloz Maria Fernanda, Perea Amarillo Raul, Vilches-Arenas Angel, Castro Laria Luisa, Maldonado Pérez Belen, Chaaro Benallal Dina, Benítez Roldán Antonio, Merino Vicente, Ramirez Gabriel, Calleja-Hernández Miguel Angel, Caunedo Álvarez Angel, Romero Gómez Manuel
aDepartment of Gastroenterology, University Virgen Macarena Hospital bDepartment of Preventive Medicine and Public Health, Virgen Macarena University Hospital cDepartment of Pharmacology, Virgen Macarena University Hospital dDepartment of Gastroenterology, Virgen del Rocío University Hospital, Institute of Biomedicie of Seville (IBIS), University of Seville, Seville, Spain.
Eur J Gastroenterol Hepatol. 2017 Nov;29(11):1290-1295. doi: 10.1097/MEG.0000000000000953.
Biological agents, such as infliximab, have transformed the outcomes of patients with immune-mediated inflammatory diseases. The advent of biosimilar treatment options such as CT-P13 promises to improve the availability of biological therapy, yet real-world switching data are currently limited. Here, we assess the effectiveness and safety of switching to CT-P13 from infliximab reference product (RP) in patients with inflammatory bowel disease.
This was a prospective single-center observational study in patients with moderate to severe Crohn's disease (CD) and ulcerative colitis (UC). All patients were switched from infliximab RP (Remicade) to CT-P13 treatment and followed up for up to 12 months. The efficacy endpoint was the change in clinical response assessed at 3-monthly intervals, according to the Harvey-Bradshaw score and partial Mayo score for patients with CD and UC, respectively. C-reactive protein (CRP) was also measured. Adverse events were monitored and recorded throughout the study.
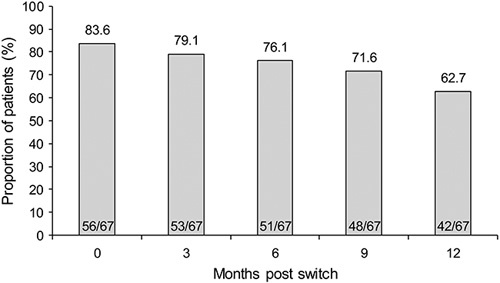
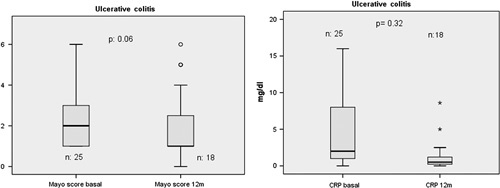
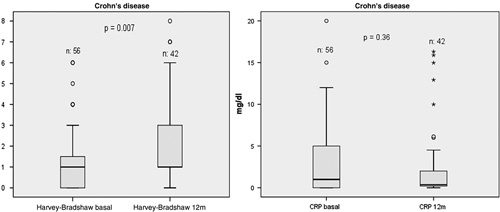
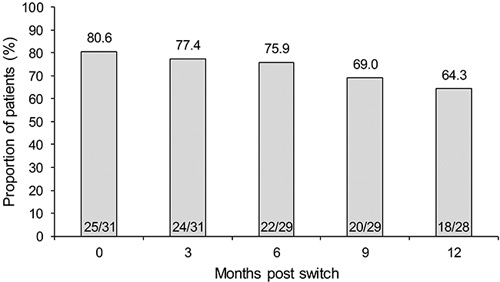
A total of 98 patients with inflammatory bowel disease (67 CD/31 UC) were included. A total of 83.6% (56/67) of patients with CD were in remission at the time of the switch and 62.7% were in remission at 12 months. The Harvey-Bradshaw score showed a significant change at 12 months (P=0.007) but no significant change was observed in median CRP at this timepoint (P=0.364). A total of 80.6% (25/31) of patients with UC were in remission at the time of the switch and 65.3% (18/28) were in remission at 12 months. No significant changes in the median partial Mayo score (P=0.058) or CRP (P=0.329) were observed at 12 months. Serious adverse events related to medication were reported in 11 (11.2%) patients.
Switching from infliximab RP to CT-P13 is efficacious and well tolerated in patients with CD or UC for up to 12 months.
英夫利昔单抗等生物制剂改变了免疫介导的炎症性疾病患者的治疗结局。CT-P13等生物类似药治疗方案的出现有望提高生物治疗的可及性,但目前真实世界中的换药数据有限。在此,我们评估炎症性肠病患者从英夫利昔单抗参比制剂(RP)换用CT-P13的有效性和安全性。
这是一项针对中度至重度克罗恩病(CD)和溃疡性结肠炎(UC)患者的前瞻性单中心观察性研究。所有患者均从英夫利昔单抗RP(类克)换用CT-P13治疗,并随访长达12个月。疗效终点是分别根据CD和UC患者的哈维-布拉德肖评分和梅奥部分评分,每3个月评估一次的临床反应变化。还检测了C反应蛋白(CRP)。在整个研究过程中监测并记录不良事件。
共纳入98例炎症性肠病患者(67例CD/31例UC)。共83.6%(56/67)的CD患者在换药时处于缓解期,12个月时62.7%处于缓解期。哈维-布拉德肖评分在12个月时出现显著变化(P=0.007),但此时CRP中位数未观察到显著变化(P=0.364)。共80.6%(25/31)的UC患者在换药时处于缓解期,12个月时65.3%(18/28)处于缓解期。12个月时梅奥部分评分中位数(P=0.058)或CRP(P=0.329)未观察到显著变化。11例(11.2%)患者报告了与药物相关的严重不良事件。
CD或UC患者从英夫利昔单抗RP换用CT-P13长达12个月时疗效良好且耐受性良好。