Organ Transplant Center, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China.
BMC Surg. 2022 Apr 7;22(1):130. doi: 10.1186/s12893-022-01574-3.
It is no consensus on the best management for patients with large hepatic hemangiomas. This study was designed to evaluate the efficacy and safety of percutaneous sclerotherapy compared to surgical resection for large hepatic hemangiomas.
A total of 89 patients with large hepatic hemangiomas from single center underwent either percutaneous sclerotherapy (n = 14) or surgical resection (n = 75) as first-line treatment was retrospectively studied, followed up for 9-24 months using ultrasound. Terms of intraoperative and postoperative information, postoperative complications, and treatment effectiveness were compared between the two groups.
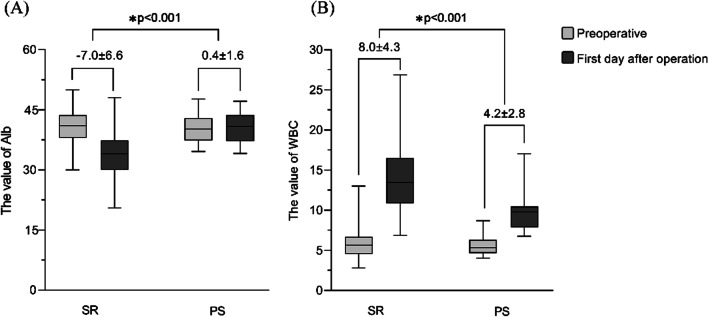
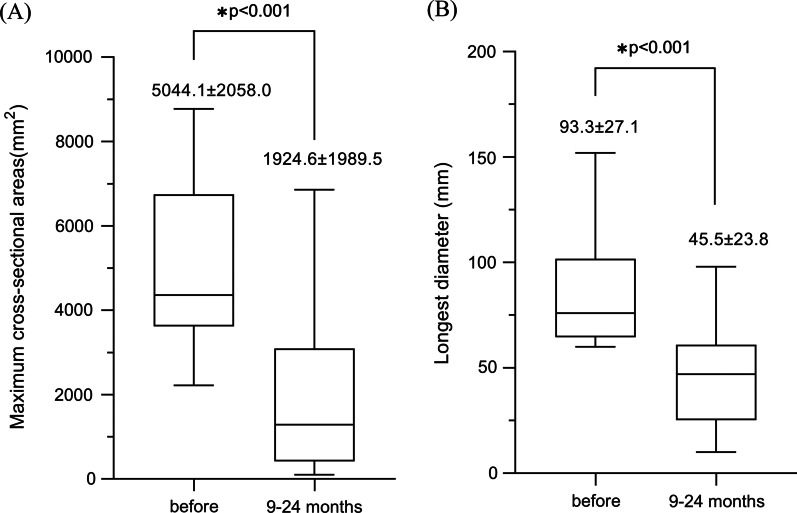
Percutaneous sclerotherapy had shorter operative time (p < 0.001), less blood loss, lower rate of prophylactic abdominal drainage (97.3% vs. 0%, p < 0.001), fewer minor complications (48.0% vs. 7.1%, p < 0.01), shorter hospital stay (p < 0.001), lower hospital cost (p < 0.001), higher Alb level (p < 0.001) and lower postoperative clinical index including ALT, AST and WBC (p < 0.001 for both) than did surgical resection. The major complications were demonstrated no significant difference between the two groups. In addition, the mean maximum cross-sectional areas of hemangioma dropped from 5044.1 ± 2058.0 mm to 1924.6 ± 1989.5 mm (65.2% reduction) during 9-24 months follow-up (p < 0.001) in the percutaneous sclerotherapy group, while all patients in the surgical resection group achieved complete response.
Percutaneous sclerotherapy is the preferred method for the treatment of large hepatic hemangioma over surgical resection when compared with the items of postoperative recovery, blood loss, complications, hospital stays, and lower hospital costs. The reduction of the maximum cross-sectional area of hepatic hemangioma in the percutaneous sclerotherapy group is satisfactory.
对于大的肝血管瘤患者,目前尚无最佳的治疗方法。本研究旨在评估经皮硬化治疗与手术切除治疗大的肝血管瘤的疗效和安全性。
回顾性分析了 89 例来自单一中心的大的肝血管瘤患者,其中 14 例行经皮硬化治疗(硬化治疗组),75 例行手术切除治疗(手术切除组)作为一线治疗。术后通过超声随访 9-24 个月。比较两组术中、术后资料、术后并发症及治疗效果。
经皮硬化治疗组的手术时间更短(p<0.001)、出血量更少(p<0.001)、预防性腹腔引流率更低(97.3% vs. 0%,p<0.001)、术后并发症发生率更低(48.0% vs. 7.1%,p<0.01)、住院时间更短(p<0.001)、住院费用更低(p<0.001)、术后白蛋白水平更高(p<0.001),丙氨酸氨基转移酶(ALT)、天门冬氨酸氨基转移酶(AST)和白细胞(WBC)等术后临床指标更低(p<0.001 均)。两组的主要并发症发生率无显著差异。此外,经皮硬化治疗组肝血管瘤最大横截面积在 9-24 个月随访期间从 5044.1±2058.0mm降至 1924.6±1989.5mm(缩小 65.2%)(p<0.001),而手术切除组所有患者均达到完全缓解。
与术后恢复、出血量、并发症、住院时间和较低的住院费用等项目相比,经皮硬化治疗是治疗大的肝血管瘤的首选方法。经皮硬化治疗组肝血管瘤最大横截面积的缩小是令人满意的。