West London Renal and Transplant Centre, Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, UK.
Chest and Allergy Clinic, St Mary's Hospital, Imperial College Healthcare NHS Trust, London, UK.
Hemodial Int. 2022 Jul;26(3):361-368. doi: 10.1111/hdi.13010. Epub 2022 Apr 7.
In patients with chronic kidney disease the risk of developing Tuberculosis is increased, while the presentation is often atypical making the diagnosis more difficult. The aim of this study is to describe the presentation of Tuberculosis in dialysis and kidney transplant patients, including the range of diagnostic approaches and the utility of different sample types.
DESIGN, SETTING, PARTICIPANTS, AND MEASUREMENTS: In this retrospective study, case records of dialysis and kidney transplant patients were reviewed, including all those treated for Tuberculosis between January 2009 and December 2020.
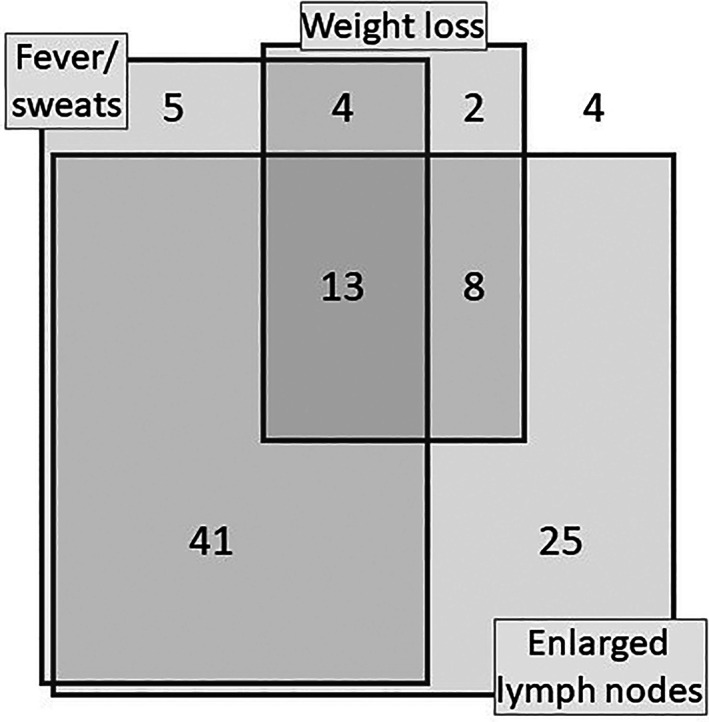
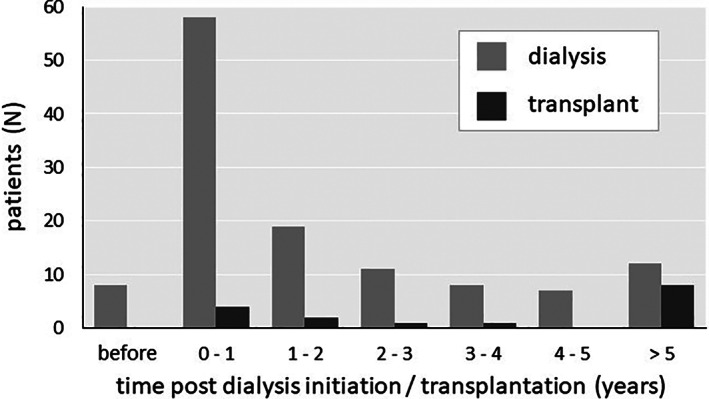
Over 12 years, there were 143 cases of Tuberculosis in 141 patients (aged 17-86, 50.4% male). Tuberculosis was most common in Asian patients (64%) and those receiving hemodialysis (82%), particularly during the first year after dialysis initiation (54% of dialysis cases). Non-pleural/pulmonary disease accounted 40% of cases, and non-organ-specific presenting features were prominent including fever, lymphadenopathy, and weight loss. The diagnosis was confirmed microbiologically or histologically in 87 cases (61%), with low sensitivity observed for many types of samples including sputum (18%) and pleural fluid (12%). Higher sensitivity was observed with tissue samples including bronchoscopic lymph node aspiration (75%) and other lymph node sampling (92%). In the 52 cases where drug sensitivities were available, resistance to a first line treatment, most commonly isoniazid, was seen in 12 cases (23%). Furthermore, 1- and 5-year survival from diagnosis were 78% and 61%, respectively. Baseline variables independently associated with poorer survival were age (OR 1.8 per decade, 95% CI 1.4-2.3), weight loss over 10% (OR 1.9, 95% CI 1.0-3.5), and a non-confirmed diagnosis (OR 1.6, 95% CI 1.2-2.1).
Tuberculosis is common in dialysis and kidney transplant patients, particularly during the first year of dialysis. Short-term mortality is high, but the diagnostic sensitivity of many types of samples is low, so that diagnosis is difficult, with treatment often initiated without confirmation. These data highlight the importance of judgment and clinical experience with this complex patient group.
慢性肾脏病患者发生结核病的风险增加,而其临床表现常不典型,导致诊断更为困难。本研究旨在描述透析和肾移植患者结核病的临床表现,包括诊断方法的范围以及不同样本类型的应用价值。
设计、地点、参与者和测量:在这项回顾性研究中,我们对透析和肾移植患者的病历进行了回顾,包括 2009 年 1 月至 2020 年 12 月期间所有接受结核病治疗的患者。
在 12 年期间,141 名患者中有 143 例结核病(年龄 17-86 岁,50.4%为男性)。亚洲患者(64%)和接受血液透析的患者(82%)结核病最为常见,尤其是在透析开始后的第一年(54%的透析病例)。非胸膜/肺部疾病占 40%,非器官特异性表现突出,包括发热、淋巴结病和体重减轻。87 例(61%)通过微生物学或组织学确诊,包括痰(18%)和胸腔积液(12%)在内的许多类型样本的敏感性较低。支气管镜下淋巴结抽吸(75%)和其他淋巴结取样(92%)的组织样本敏感性较高。在 52 例可获得药敏结果的病例中,一线治疗耐药,最常见的是异烟肼,有 12 例(23%)。此外,从诊断到 1 年和 5 年的生存率分别为 78%和 61%。与生存率较差相关的基线变量包括年龄(每增加 10 年,OR 1.8,95%CI 1.4-2.3)、体重减轻超过 10%(OR 1.9,95%CI 1.0-3.5)和未确诊(OR 1.6,95%CI 1.2-2.1)。
结核病在透析和肾移植患者中很常见,尤其是在透析的第一年。短期死亡率较高,但许多类型样本的诊断敏感性较低,导致诊断困难,治疗通常在未确诊的情况下开始。这些数据强调了对这类复杂患者群体的判断和临床经验的重要性。