Paris Fire Brigade, Emergency Medicine dpt, 1 place Jules Renard, 75017 Paris, France.
Paris Fire Brigade, Emergency Medicine dpt, 1 place Jules Renard, 75017 Paris, France.
Am J Emerg Med. 2022 Jun;56:133-136. doi: 10.1016/j.ajem.2022.03.059. Epub 2022 Apr 1.
There exists a need for prognostic tools for the early identification of COVID-19 patients requiring intensive care unit (ICU) admission and mortality. Here we investigated the association between a clinical (initial prehospital shock index (SI)) and biological (initial prehospital lactatemia) tool and the ICU admission and 30-day mortality among COVID-19 patients cared for in the prehospital setting.
We retrospectively analysed COVID-19 patients initially cared for by a Paris Fire Brigade advanced (ALS) or basic life support (BLS) team in the prehospital setting between 2020, March 08th and 2020, May 30th. We assessed the association between prehospital SI and prehospital lactatemia and ICU admission and mortality using logistic regression model analysis after propensity score matching with Inverse Probability Treatment Weighting (IPTW) method. Covariates included in the IPTW propensity analysis were: age, sex, body mass index (BMI), initial respiratory rate (iRR), initial pulse oximetry without (SpO2i) and with oxygen supplementation (SpO2i.O2), initial Glasgow coma scale (GCSi) value, initial prehospital SI and initial prehospital lactatemia.
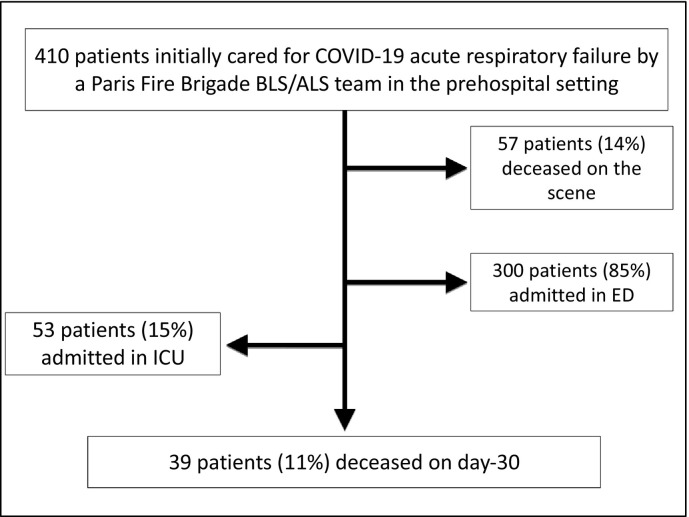
We analysed 410 consecutive COVID-19 patients [254 males (62%); mean age, 64 ± 18 years]. Fifty-seven patients (14%) deceased on the scene, of whom 41 (72%) were male and were significantly older (71 ± 12 years vs. 64 ± 19 years; P 〈10). Fifty-three patients (15%) were admitted in ICU and 39 patients (11%) were deceased on day-30. The mean prehospital SI value was 1.5 ± 0.4 and the mean prehospital lactatemia was 2.0 ± 1.7 mmol.l. Multivariate logistic regression analysis on matched population after IPTW propensity analysis reported a significant association between ICU admission and age (adjusted Odd-Ratio (aOR), 0.90; 95% confidence interval (95%CI): 0.93-0.98;p = 10), SpO2i.O2 (aOR, 1.10; 95%CI: 1.02-1.20;p = 0.002) and BMI (aOR, 1.09; 95% CI: 1.03-1.16;p = 0.02). 30-day mortality was significantly associated with SpO2i.O2 (aOR, 0.92; 95% CI: 0.87-0.98;p = 0.01 P < 10) and GCSi (aOR, 0.90; 95% CI: 0.82-0.99;p = 0.04). Neither prehospital SI nor prehospital lactatemia were associated with ICU admission and 30-day mortality.
Neither prehospital initial SI nor lactatemia were associated with ICU admission and 30-day mortality among COVID-19 patients initially cared for by a Paris Fire Brigade BLS or ALS team. Further prospective studies are needed to confirm these preliminary results.
需要有预测工具来早期识别需要入住重症监护病房(ICU)和死亡的 COVID-19 患者。在这里,我们研究了临床(初始院前休克指数(SI))和生物学(初始院前乳酸性血症)工具与 COVID-19 患者入住 ICU 和 30 天死亡率之间的关联,这些患者在院前环境中接受治疗。
我们回顾性分析了 2020 年 3 月 8 日至 2020 年 5 月 30 日期间,巴黎消防队高级(ALS)或基础生命支持(BLS)团队在院前环境中最初照顾的 COVID-19 患者。我们使用逻辑回归模型分析,在校正倾向评分匹配的逆概率处理权重(IPTW)方法后,评估了院前 SI 和院前乳酸性血症与 ICU 入院和死亡率之间的关联。纳入 IPTW 倾向分析的协变量包括:年龄、性别、体重指数(BMI)、初始呼吸频率(iRR)、初始脉搏血氧饱和度(SpO2i)和吸氧时的 SpO2i(SpO2i.O2)、初始格拉斯哥昏迷量表(GCSi)值、初始院前 SI 和初始院前乳酸性血症。
我们分析了 410 例连续的 COVID-19 患者[254 名男性(62%);平均年龄 64 ± 18 岁]。57 名患者(14%)在现场死亡,其中 41 名(72%)为男性,且年龄明显较大(71 ± 12 岁比 64 ± 19 岁;P〈10)。53 名患者(15%)被收治 ICU,39 名患者(11%)在第 30 天死亡。平均院前 SI 值为 1.5 ± 0.4,平均院前乳酸性血症为 2.0 ± 1.7 mmol.l。经 IPTW 倾向分析后对匹配人群进行多变量逻辑回归分析报告 ICU 入院与年龄(调整后的优势比(aOR),0.90;95%置信区间(95%CI):0.93-0.98;p = 10)、SpO2i.O2(aOR,1.10;95%CI:1.02-1.20;p = 0.002)和 BMI(aOR,1.09;95%CI:1.03-1.16;p = 0.02)显著相关。30 天死亡率与 SpO2i.O2(aOR,0.92;95%CI:0.87-0.98;p = 0.01)和 GCSi(aOR,0.90;95%CI:0.82-0.99;p = 0.04)显著相关。院前 SI 和乳酸性血症均与 ICU 入院和 30 天死亡率无关。
巴黎消防队 BLS 或 ALS 团队最初照顾的 COVID-19 患者中,院前初始 SI 或乳酸性血症均与 ICU 入院和 30 天死亡率无关。需要进一步的前瞻性研究来证实这些初步结果。