Institute of Biomedical Ethics and History of Medicine (IBME), University of Zurich, Winterthurerstr. 30, 8006, Zurich, Switzerland.
Med Health Care Philos. 2022 Sep;25(3):351-360. doi: 10.1007/s11019-022-10079-y. Epub 2022 Apr 10.
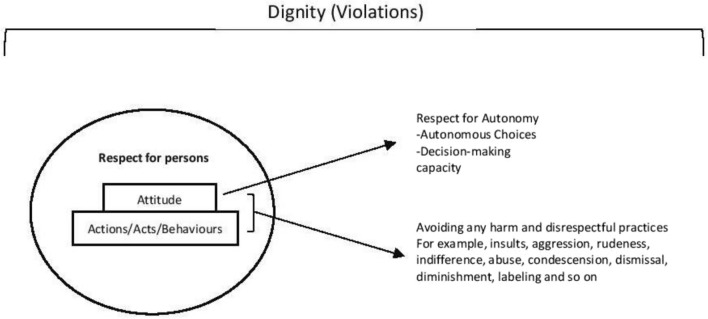
In everyday conversations, professional codes, policy debates, and academic literature, the concept of respect is referred to frequently. Bioethical arguments in recent decades equate the idea of respect for persons with individuals who are capable of autonomous decision-making, with the focus being explicitly on 'autonomy,' 'capacity,' or 'capability.' In much of bioethics literature, respect for persons is replaced by respect for autonomy. Though the unconditional respect for persons and their autonomy (irrespective of actual decision-making capacity) is established in Kantian bioethics, current argument and debates often revolve around a thin concept of autonomy, focusing on capacity and capability: persons are owed respect because they are 'rational beings' or with a focus on 'agency' and 'decision-making abilities.' However, these aspects alone are insufficient while engaging the concept of respect for persons, particularly in healthcare settings. This paper sets out to explore if the concept of respect for persons-as opposed to a thin concept of autonomy-could help us engage better in healthcare practices. We shall probe the practical value of the experiential aspect of respect-understood as the recognition of persons as respect-worthy through certain dispositions and deliberative acts-by reflecting on instances in clinical practice that tend to be dismissed as negligible or even unavoidable in a stressful environment such as a busy hospital. We shall argue that these instances are far from trivial but carry moral significance and express an unacceptable-disrespectful-attitude that can compromise the moral habitus in hospital settings. In our conclusion, we call for practicing recognition respect in the health professional-patient encounter by focussing on manners, attitudes, and behaviors. Furthermore, we call for continuous medical ethics education programs to address the moral significance of disrespectful behaviors and their manifestations in particular socio-cultural contexts.
在日常对话、专业规范、政策辩论和学术文献中,经常提到“尊重”的概念。近几十年来,生物伦理学的论点将尊重人的概念等同于能够自主决策的个人,其重点明确放在“自主性”、“能力”或“能力”上。在生物伦理学文献中,尊重人被尊重自主权所取代。虽然无条件尊重人和他们的自主权(无论实际决策能力如何)在康德式的生物伦理学中是既定的,但当前的论点和辩论往往围绕着一个薄弱的自主权概念展开,关注能力和能力:人们应该得到尊重,因为他们是“理性的存在”,或者关注“能动性”和“决策能力”。然而,在涉及尊重人的概念时,仅这些方面是不够的,特别是在医疗保健环境中。本文旨在探讨尊重人的概念(而不是薄弱的自主权概念)是否有助于我们更好地参与医疗保健实践。我们将探讨尊重人的经验方面的实际价值——通过某些态度和审议行为将人理解为值得尊重的——通过反思临床实践中的实例,这些实例在紧张的环境(如繁忙的医院)中往往被视为微不足道甚至不可避免的。我们将认为,这些情况远非微不足道,而是具有道德意义,并表达了一种不可接受的、不尊重的态度,这种态度可能会损害医院环境中的道德习惯。在我们的结论中,我们呼吁通过关注举止、态度和行为,在医患互动中实践认可尊重。此外,我们呼吁继续开展医学伦理教育计划,以解决不尊重行为及其在特定社会文化背景下的表现的道德意义。