Kim Ju Youn, Jeong Dong Seop, Park Seung-Jung, Park Kyoung-Min, Kim June Soo, On Young Keun
Division of Cardiology, Department of Internal Medicine, Samsung Medical Center, Heart Vascular and Stroke Institute, Sungkyunkwan University School of Medicine, Seoul, South Korea.
Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea.
Front Cardiovasc Med. 2022 Mar 31;9:853299. doi: 10.3389/fcvm.2022.853299. eCollection 2022.
Atrial fibrillation (AF) is associated with an increased ischemic stroke, and the left atrial appendage (LAA) represents the main source of thrombus formation. We evaluated the long-term efficacy of surgical thoracoscopic LAA occlusion during total thoracoscopic ablation of AF to prevent the stroke and anticoagulation strategy after surgery.
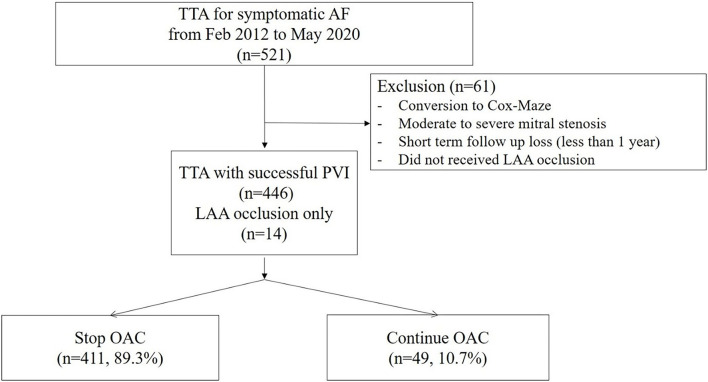
Patients who underwent total thoracoscopic ablation for AF, from February 2012 to May 2020, were included; Patients who did not receive LAA occlusion were excluded. We evaluated the development of thromboembolism in these patients.
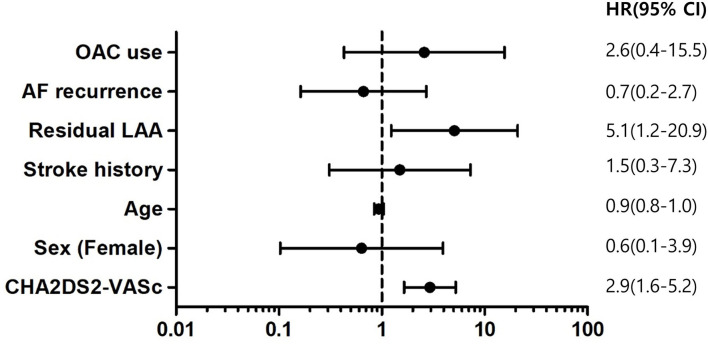
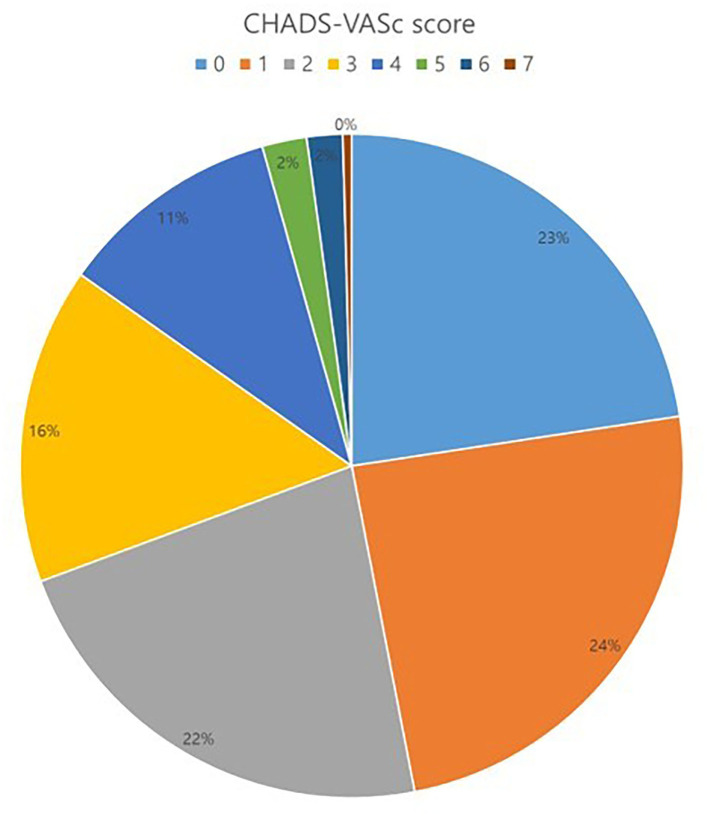
The total number of 460 patients [mean age, 57.1 ± 9.2 years; 400 (87.0%) males] were included in the study. The mean follow-up duration was 44.8 months. The mean CHADS-VASc score was 1.9 ± 1.6. Median OAC duration was 109.5 days after the surgery, and the final number of patients who discontinued OAC were 411 (89.3%) in total. Anticoagulation discontinuation rate according to CHADS-VASc score are as follows; (i) 0 = 99.0%; (ii) 1 = 98.2%; and (iii) ≥2 = 81.3%. The annualized incidence rate of ischemic stroke was 0.78%/year, showing a 73% risk reduction compared with the CHADS-VASc predicted rate without anticoagulation. The hazard ratio for ischemic stroke according to previous stroke history was 1.5 [95% confidential interval (CI) 0.3-7.3, = 0.62], and that of remnant LAA was 5.1 (1.2-20.9, = 0.02).
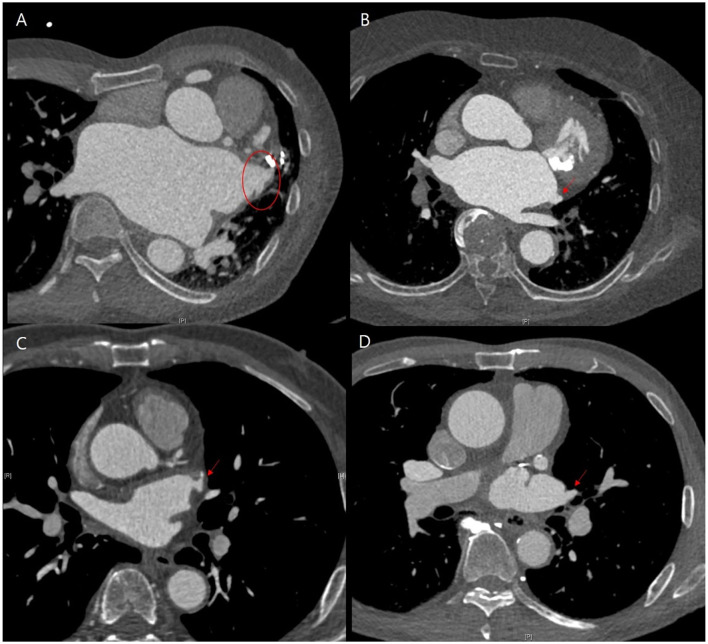
Thoracoscopic LAA occlusion during total thoracoscopic ablation of AF was effective to prevent ischemic stroke. Most patients could discontinue OAC therapy after the procedure. Patients who had a residual trabeculated LAA, or peri-occluder pouch in follow-up CT need to maintain OAC therapy even after LAA occlusion.
心房颤动(AF)与缺血性卒中风险增加相关,左心耳(LAA)是血栓形成的主要来源。我们评估了在全胸腔镜下房颤消融术中进行手术胸腔镜下LAA封堵预防卒中的长期疗效以及术后抗凝策略。
纳入2012年2月至2020年5月期间接受全胸腔镜下房颤消融术的患者;排除未接受LAA封堵的患者。我们评估了这些患者血栓栓塞的发生情况。
本研究共纳入460例患者[平均年龄57.1±9.2岁;400例(87.0%)为男性]。平均随访时间为44.8个月。平均CHADS-VASc评分为1.9±1.6。术后OAC(口服抗凝药)的中位使用时间为109.5天,最终共有411例(89.3%)患者停用OAC。根据CHADS-VASc评分的抗凝停药率如下:(i)0分=99.0%;(ii)1分=98.2%;(iii)≥2分=81.3%。缺血性卒中的年化发病率为0.78%/年,与未抗凝时CHADS-VASc预测的发病率相比,风险降低了73%。根据既往卒中史,缺血性卒中的风险比为1.5[95%置信区间(CI)0.3 - 7.3,P = 0.62],残留LAA者的风险比为5.1(1.2 - 20.9,P = 0.02)。
在全胸腔镜下房颤消融术中进行胸腔镜下LAA封堵可有效预防缺血性卒中。大多数患者术后可停用OAC治疗。随访CT显示有残留小梁状LAA或封堵器周围袋状结构的患者,即使在LAA封堵后也需要维持OAC治疗。