Lee Terry, Cheng Matthew P, Vinh Donald C, Lee Todd C, Tran Karen C, Winston Brent W, Sweet David, Boyd John H, Walley Keith R, Haljan Greg, McGeer Allison, Lamontagne François, Fowler Robert, Maslove David, Singer Joel, Patrick David M, Marshall John C, Burns Kevin D, Murthy Srinivas, Mann Puneet K, Hernandez Geraldine, Donohoe Kathryn, Rocheleau Genevieve, Russell James A
Centre for Health Evaluation and Outcome Sciences (T. Lee, Singer), St. Paul's Hospital, University of British Columbia, Vancouver, BC; Division of Infectious Diseases (Cheng, Vinh, T.C. Lee), Department of Medicine, McGill University Health Centre, Montréal, Que.; Division of General Internal Medicine (Tran), Vancouver General Hospital; University of British Columbia (Tran, Sweet, Patrick, Murthy), Vancouver, BC; Departments of Critical Care Medicine (Winston), Medicine (Winston) and Biochemistry and Molecular Biology (Winston), Foothills Medical Centre; University of Calgary (Winston), Calgary, Alta.; Division of Critical Care Medicine (Sweet), Vancouver General Hospital; Centre for Heart Lung Innovation (Boyd, Walley, Russell) and Division of Critical Care Medicine (Boyd, Walley, Russell), St. Paul's Hospital, University of British Columbia, Vancouver, BC; Department of Medicine (Haljan), Surrey Memorial Hospital, Surrey, BC; Mount Sinai Hospital (McGeer); University of Toronto (McGeer), Toronto, Ont.; Université de Sherbrooke (Lamontagne), Sherbrooke, Que.; Sunnybrook Health Sciences Centre (Fowler), Toronto, Ont.; Department of Critical Care (Maslove), Kingston General Hospital and Queen's University, Kingston, Ont.; British Columbia Centre for Disease Control (Patrick), Vancouver, BC; Department of Surgery (Marshall), St. Michael's Hospital, Toronto, Ont.; Division of Nephrology (Burns), Department of Medicine, Ottawa Hospital Research Institute, University of Ottawa, Ottawa, Ont.; BC Children's Hospital (Murthy); Black Tusk Research Group (Mann, Hernandez, Donohoe, Rocheleau), Vancouver, BC.
Centre for Health Evaluation and Outcome Sciences (T. Lee, Singer), St. Paul's Hospital, University of British Columbia, Vancouver, BC; Division of Infectious Diseases (Cheng, Vinh, T.C. Lee), Department of Medicine, McGill University Health Centre, Montréal, Que.; Division of General Internal Medicine (Tran), Vancouver General Hospital; University of British Columbia (Tran, Sweet, Patrick, Murthy), Vancouver, BC; Departments of Critical Care Medicine (Winston), Medicine (Winston) and Biochemistry and Molecular Biology (Winston), Foothills Medical Centre; University of Calgary (Winston), Calgary, Alta.; Division of Critical Care Medicine (Sweet), Vancouver General Hospital; Centre for Heart Lung Innovation (Boyd, Walley, Russell) and Division of Critical Care Medicine (Boyd, Walley, Russell), St. Paul's Hospital, University of British Columbia, Vancouver, BC; Department of Medicine (Haljan), Surrey Memorial Hospital, Surrey, BC; Mount Sinai Hospital (McGeer); University of Toronto (McGeer), Toronto, Ont.; Université de Sherbrooke (Lamontagne), Sherbrooke, Que.; Sunnybrook Health Sciences Centre (Fowler), Toronto, Ont.; Department of Critical Care (Maslove), Kingston General Hospital and Queen's University, Kingston, Ont.; British Columbia Centre for Disease Control (Patrick), Vancouver, BC; Department of Surgery (Marshall), St. Michael's Hospital, Toronto, Ont.; Division of Nephrology (Burns), Department of Medicine, Ottawa Hospital Research Institute, University of Ottawa, Ottawa, Ont.; BC Children's Hospital (Murthy); Black Tusk Research Group (Mann, Hernandez, Donohoe, Rocheleau), Vancouver, BC
CMAJ Open. 2022 Apr 19;10(2):E379-E389. doi: 10.9778/cmajo.20210216. Print 2022 Apr-Jun.
There have been multiple waves in the COVID-19 pandemic in many countries. We sought to compare mortality and respiratory, cardiovascular and renal dysfunction between waves in 3 Canadian provinces.
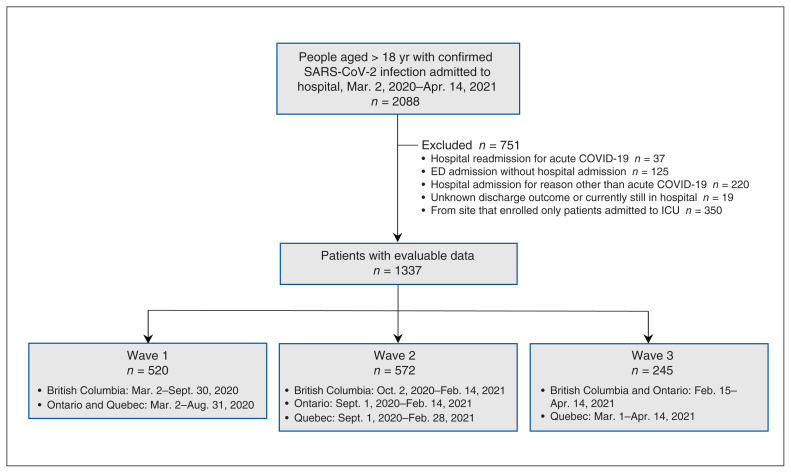
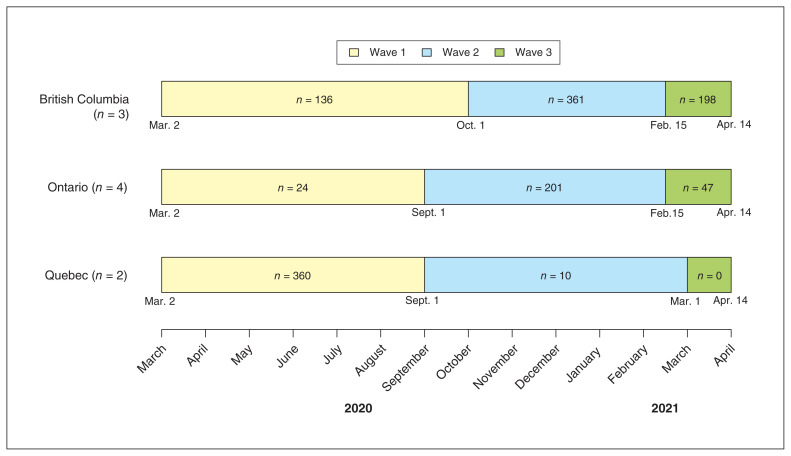
We conducted a substudy of the ARBs CORONA I study, a multicentre Canadian pragmatic observational cohort study that examined the association of pre-existing use of angiotensin receptor blockers with outcomes in adults admitted to hospital with acute COVID-19 up to April 2021 from 9 community and teaching hospitals in 3 Canadian provinces (British Columbia, Ontario and Quebec). We excluded emergency department admissions without hospital admission, readmissions and admissions for another reason. We used logistic and 0-1-inflated β regression models to compare 28-day and in-hospital mortality, and the use of invasive mechanical ventilation, vasopressors and renal replacement therapy (RRT) between the first 3 waves of the COVID-19 pandemic in these provinces.
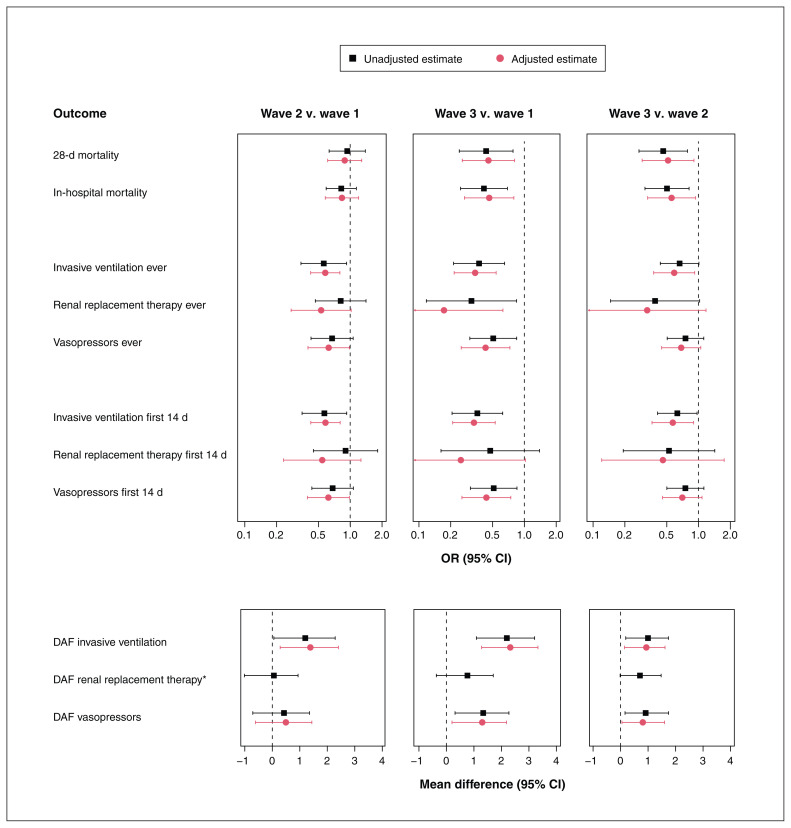
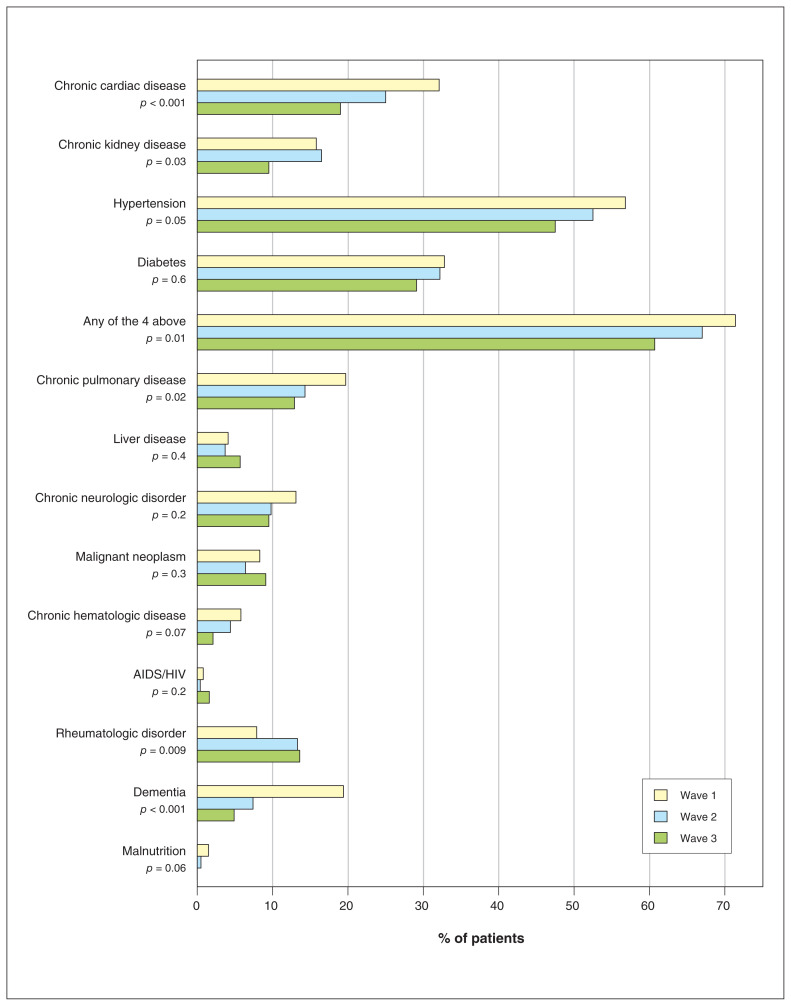
A total of 520, 572 and 245 patients in waves 1, 2 and 3, respectively, were included. Patients in wave 3 were on average younger and had fewer comorbidities than those in waves 1 and 2. The unadjusted 28-day mortality rate was significantly lower in wave 3 (7.8%) than in wave 1 (18.3%) (odds ratio [OR] 0.43, 95% confidence interval [CI] 0.24-0.78) and wave 2 (16.3%) (OR 0.46, 95% CI 0.27-0.79). After adjustment for differences in baseline characteristics, the difference in 28-day mortality remained significant (adjusted OR wave 3 v. wave 1: 0.46, 95% CI 0.26-0.81; wave 3 v. wave 2: 0.52, 95% CI 0.29-0.91). In-hospital mortality findings were similar. Use of invasive mechanical ventilation or vasopressors was less common in waves 2 and 3 than in wave 1, and use of RRT was less common in wave 3 than in wave 1.
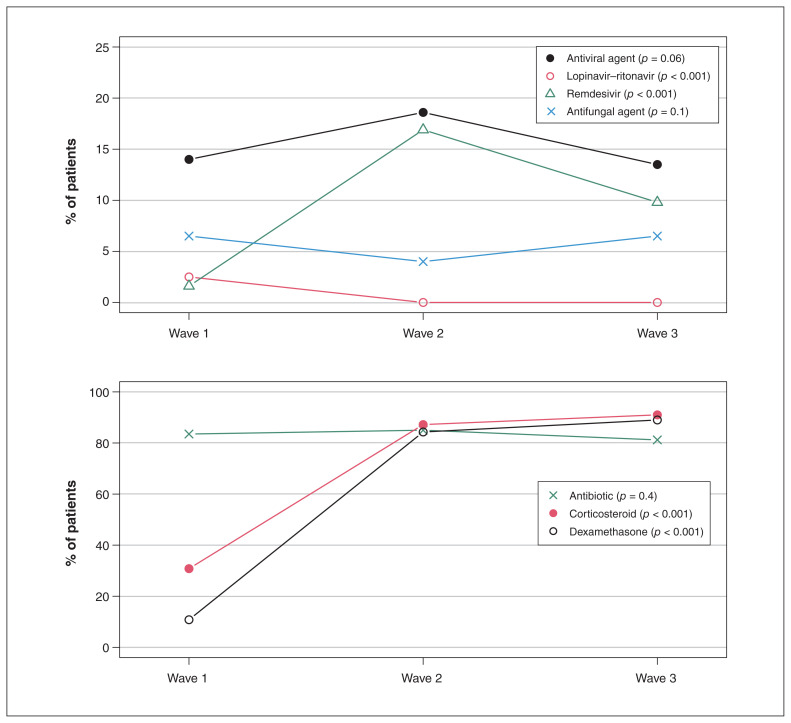
Severity of illness decreased (lower mortality and less use of organ support) across waves among patients admitted to hospital with acute COVID-19, possibly owing to changes in patient demographic characteristics and management, such as increased use of dexamethasone. Continued application of proven therapies may further improve outcomes.
ClinicalTrials.gov, no. NCT04510623.
在许多国家,新冠疫情已出现多波高峰。我们试图比较加拿大3个省份不同波次疫情期间的死亡率以及呼吸、心血管和肾功能障碍情况。
我们对ARBs CORONA I研究进行了一项子研究,这是一项加拿大多中心实用性观察性队列研究,旨在探讨既往使用血管紧张素受体阻滞剂与2021年4月前因急性新冠肺炎入住9家社区和教学医院(位于加拿大3个省份:不列颠哥伦比亚省、安大略省和魁北克省)的成年患者结局之间的关联。我们排除了未住院的急诊科入院患者、再次入院患者以及因其他原因入院的患者。我们使用逻辑回归模型和0-1膨胀β回归模型来比较这些省份新冠疫情前三波期间的28天死亡率和住院死亡率,以及有创机械通气、血管活性药物和肾脏替代治疗(RRT)的使用情况。
分别纳入了第1波、第2波和第3波的520例、572例和245例患者。与第1波和第2波的患者相比,第3波的患者平均年龄更小,合并症更少。第3波的未调整28天死亡率(7.8%)显著低于第1波(18.3%)(优势比[OR]0.43,95%置信区间[CI]0.24-0.78)和第2波(16.3%)(OR 0.46,95%CI 0.27-0.79)。在对基线特征差异进行调整后,28天死亡率的差异仍然显著(第3波与第1波比较的调整后OR:0.46,95%CI 0.26-0.81;第3波与第2波比较的调整后OR:0.52,95%CI 0.29-0.91)。住院死亡率的结果相似。第2波和第3波中使用有创机械通气或血管活性药物的情况比第1波少见,第3波中使用RRT的情况比第1波少见。
因急性新冠肺炎住院的患者在不同波次疫情期间疾病严重程度下降(死亡率降低且器官支持使用减少),这可能归因于患者人口统计学特征和管理方式的变化,如地塞米松使用增加。持续应用已证实有效的治疗方法可能会进一步改善结局。
ClinicalTrials.gov,编号NCT04510623。