Laboratory for Experimental Cardiology, Department of Cardiology, University Medical Centre Utrecht, Utrecht, The Netherlands.
Julius Center for Health Sciences and Primary Care Complex Genetics Section, Universitair Medical Center Utrecht, Utrecht, The Netherlands.
Open Heart. 2022 Apr;9(1). doi: 10.1136/openhrt-2021-001900.
Uncertainty about the benefit of (high-intensity) statins for women remains due to under-representation of women in primary prevention trials and scarcity of sex-stratified data. This study evaluates the sex-specific relation between statin treatment and survival and the additional benefit of high-intensity statins.
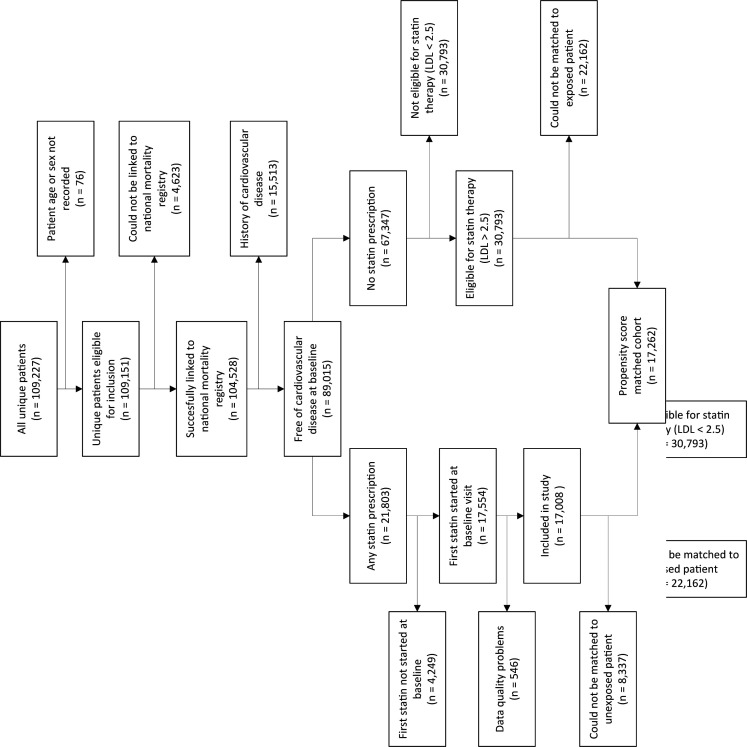
Electronic health record data from 47 801 patients (17 008 statin users and 30 793 non-users) without prior cardiovascular disease were extracted from thirteen Dutch outpatient cardiology clinics. Patients prescribed statins at baseline were propensity-score matched to those eligible for statin therapy (low-density lipoprotein >2.5 mmol/L) without a statin prescription. Statins were divided into low-intensity and high-intensity according to Dutch guidelines. Mortality data were obtained via linkage to the national mortality registry. Cox regression was used to evaluate the relationship between statin prescription and intensity and all-cause and cardiovascular mortality.
Propensity score matching created a cohort of 8631 statin users and 8631 non-users. 35% of women and 28% of men received a low-intensity statin. The beneficial effect of statins on both all-cause and cardiovascular mortality was stronger in women (HR 0.66, 95% CI 0.58 to 0.74 and HR 0.55, 95% CI 0.39 to 0.71, respectively) than in men (HR 0.89, 95% CI 0.81 to 0.95 and HR 0.93, 95% CI 0.77 to 1.08, respectively). High-intensity statins conferred modest protection against all-cause mortality (HR 0.94, 95% CI 0.88 to 1.00) and cardiovascular mortality (HR 0.86, 95% CI 0.74 to 0.98) in both sexes.
The protective effect of primary prevention statins was stronger in women than men for both all-cause and cardiovascular mortality. High-intensity statins conferred a modest additional benefit in both sexes. Statins seem to be effective regardless of treatment intensity, especially in women.
由于女性在一级预防试验中的代表性不足以及缺乏按性别分层的数据,因此(高强度)他汀类药物对女性的益处仍存在不确定性。本研究评估了他汀类药物治疗与生存之间的性别特异性关系,以及高强度他汀类药物的额外获益。
从 13 家荷兰门诊心脏病学诊所的电子健康记录中提取了 47801 名无既往心血管疾病的患者(17008 名他汀类药物使用者和 30793 名非使用者)的数据。根据荷兰指南,根据基线时开处方他汀类药物的患者与符合他汀类药物治疗条件(低密度脂蛋白 >2.5mmol/L)但未开具他汀类药物处方的患者进行倾向评分匹配。根据荷兰指南将他汀类药物分为低强度和高强度。通过与国家死亡率登记处的链接获得死亡率数据。使用 Cox 回归评估他汀类药物处方和强度与全因和心血管死亡率之间的关系。
倾向评分匹配创建了一个包含 8631 名他汀类药物使用者和 8631 名非使用者的队列。35%的女性和 28%的男性接受了低强度他汀类药物治疗。与男性(HR 0.89,95%CI 0.81 至 0.95 和 HR 0.93,95%CI 0.77 至 1.08)相比,女性的他汀类药物对全因和心血管死亡率的有益影响更强(HR 0.66,95%CI 0.58 至 0.74 和 HR 0.55,95%CI 0.39 至 0.71)。高强度他汀类药物对两性的全因死亡率(HR 0.94,95%CI 0.88 至 1.00)和心血管死亡率(HR 0.86,95%CI 0.74 至 0.98)均有适度的保护作用。
一级预防他汀类药物对女性的全因和心血管死亡率的保护作用强于男性。高强度他汀类药物对两性均有适度的额外获益。他汀类药物似乎无论治疗强度如何都有效,尤其是对女性。