Coronavirus Disease 2019 Response Team, Centers for Disease Control and Prevention, Atlanta, GA; Epidemic Intelligence Service, Centers for Disease Control and Prevention, Atlanta, GA.
Coronavirus Disease 2019 Response Team, Centers for Disease Control and Prevention, Atlanta, GA.
J Pediatr. 2022 Aug;247:29-37.e7. doi: 10.1016/j.jpeds.2022.04.032. Epub 2022 Apr 18.
To assess the household secondary infection risk (SIR) of B.1.1.7 (Alpha) and non-Alpha lineages of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) among children.
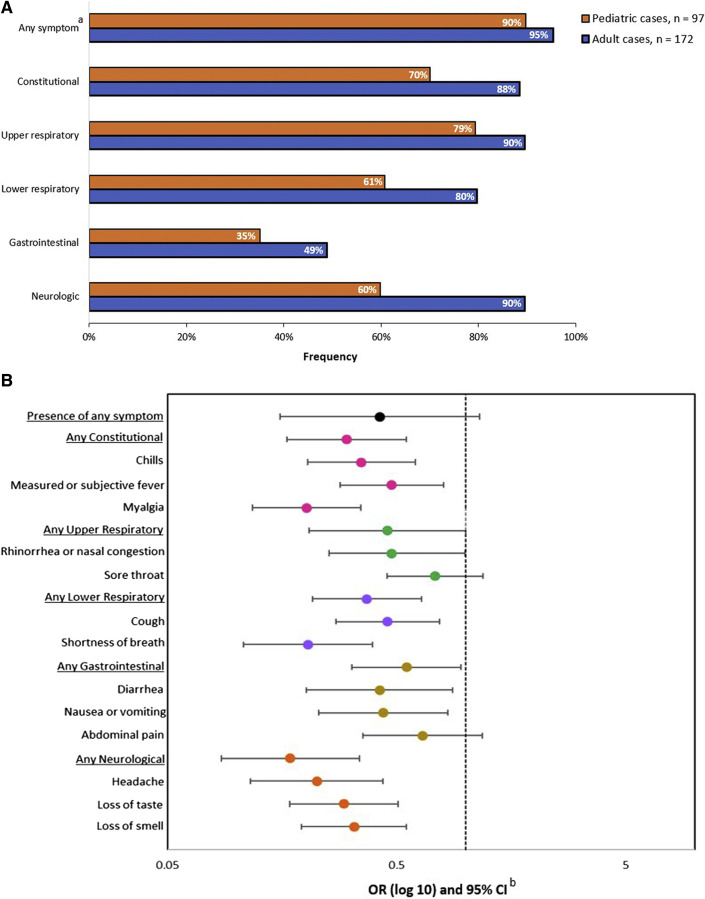
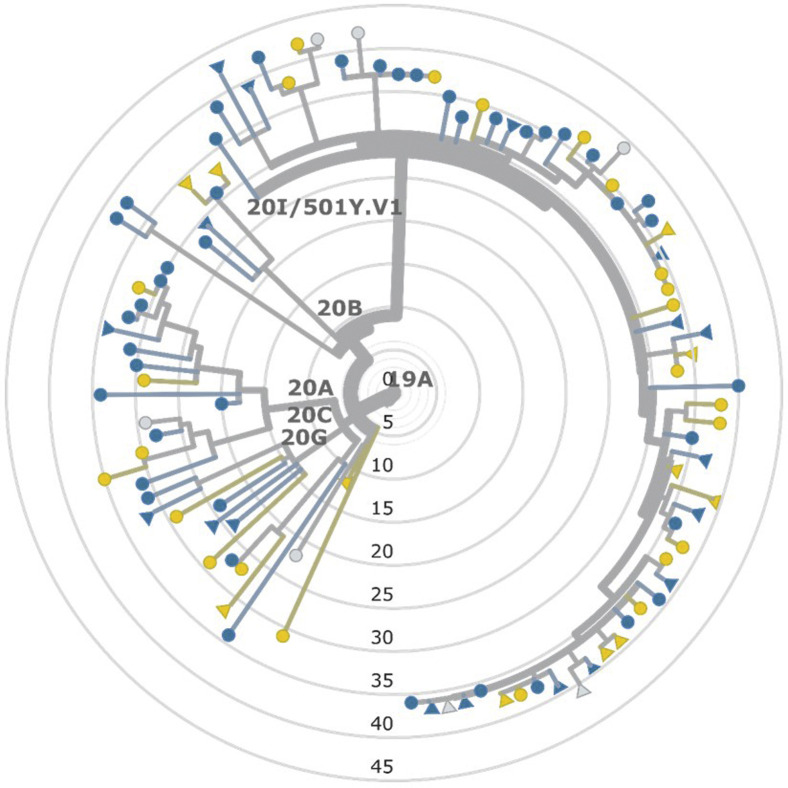
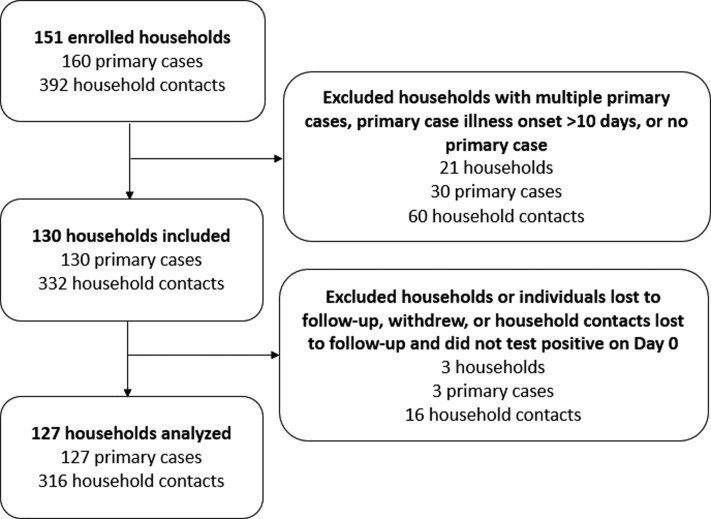
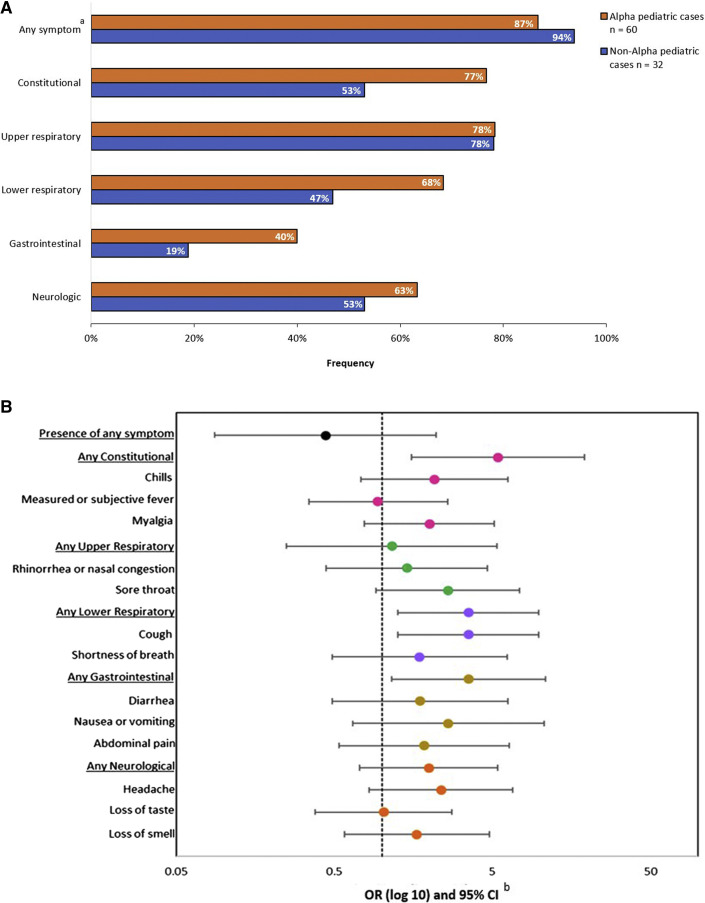
During January to April 2021, we prospectively followed households with a SARS-CoV-2 infection. We collected questionnaires, serial nasopharyngeal swabs for reverse transcription polymerase chain reaction testing and whole genome sequencing, and serial blood samples for serology testing. We calculated SIRs by primary case age (pediatric vs adult), household contact age, and viral lineage. We evaluated risk factors associated with transmission and described symptom profiles among children.
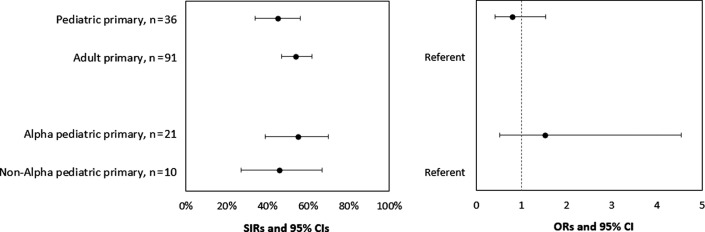
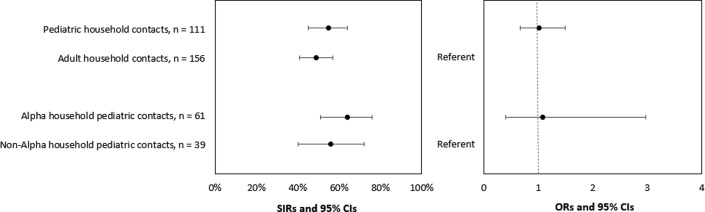
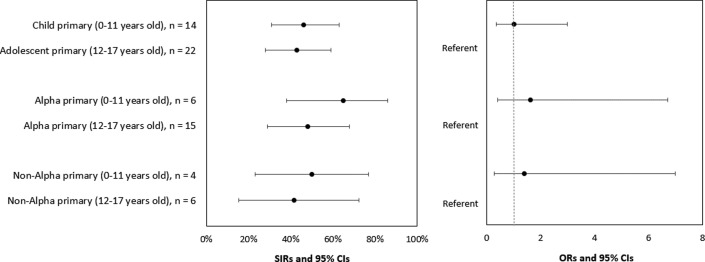
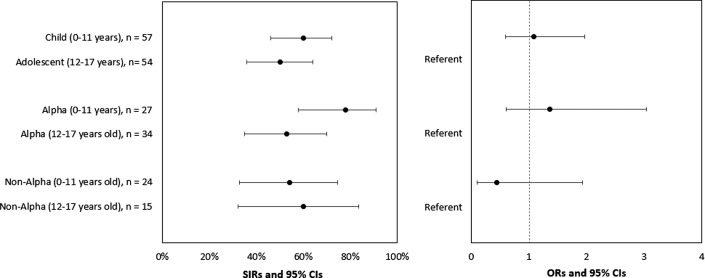
Among 36 households with pediatric primary cases, 21 (58%) had secondary infections. Among 91 households with adult primary cases, 51 (56%) had secondary infections. SIRs among pediatric and adult primary cases were 45% and 54%, respectively (OR, 0.79; 95% CI, 0.41-1.54). SIRs among pediatric primary cases with Alpha and non-Alpha lineage were 55% and 46%, respectively (OR, 1.52; 95% CI, 0.51-4.53). SIRs among pediatric and adult household contacts were 55% and 49%, respectively (OR, 1.01; 95% CI, 0.68-1.50). Among pediatric contacts, no significant differences in the odds of acquiring infection by demographic or household characteristics were observed.
Household transmission of SARS-CoV-2 from children and adult primary cases to household members was frequent. The risk of secondary infection was similar among child and adult household contacts. Among children, household transmission of SARS-CoV-2 and the risk of secondary infection was not influenced by lineage. Continued mitigation strategies (eg, masking, physical distancing, vaccination) are needed to protect at-risk groups regardless of virus lineage circulating in communities.
评估儿童中 B.1.1.7(阿尔法)和严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)非阿尔法谱系的家庭二次感染风险(SIR)。
在 2021 年 1 月至 4 月期间,我们前瞻性地随访了 SARS-CoV-2 感染的家庭。我们收集了问卷、用于逆转录聚合酶链反应检测和全基因组测序的连续鼻咽拭子以及用于血清学检测的连续血液样本。我们根据主要病例年龄(儿科与成人)、家庭接触年龄和病毒谱系计算了 SIR。我们评估了与传播相关的危险因素,并描述了儿童的症状特征。
在 36 个有儿科原发性病例的家庭中,有 21 个(58%)发生了继发性感染。在 91 个有成人原发性病例的家庭中,有 51 个(56%)发生了继发性感染。儿科和成人原发性病例的 SIR 分别为 45%和 54%(OR,0.79;95%CI,0.41-1.54)。儿科原发性病例中阿尔法和非阿尔法谱系的 SIR 分别为 55%和 46%(OR,1.52;95%CI,0.51-4.53)。儿科和成人家庭接触者的 SIR 分别为 55%和 49%(OR,1.01;95%CI,0.68-1.50)。在儿科接触者中,在人口统计学或家庭特征方面,感染的几率没有显著差异。
儿童和成人原发性病例向家庭成员传播 SARS-CoV-2 的家庭传播很常见。儿童和成人家庭接触者二次感染的风险相似。在儿童中,SARS-CoV-2 的家庭传播和二次感染的风险不受谱系影响。无论社区中流行的病毒谱系如何,都需要继续采取缓解策略(例如,戴口罩、保持身体距离、接种疫苗)来保护高危人群。