Wieczorek Aleksandra, Manzitti Carla, Garaventa Alberto, Gray Juliet, Papadakis Vassilios, Valteau-Couanet Dominique, Zachwieja Katarzyna, Poetschger Ulrike, Pribill Ingrid, Fiedler Stefan, Ladenstein Ruth, Lode Holger N
Pediatric Hematology Oncology, Jagiellonian University Medical College, 30-663 Krakow, Poland.
Oncology Unit, IRCCS Istituto Giannina Gaslini, 16147 Genova, Italy.
Cancers (Basel). 2022 Apr 10;14(8):1919. doi: 10.3390/cancers14081919.
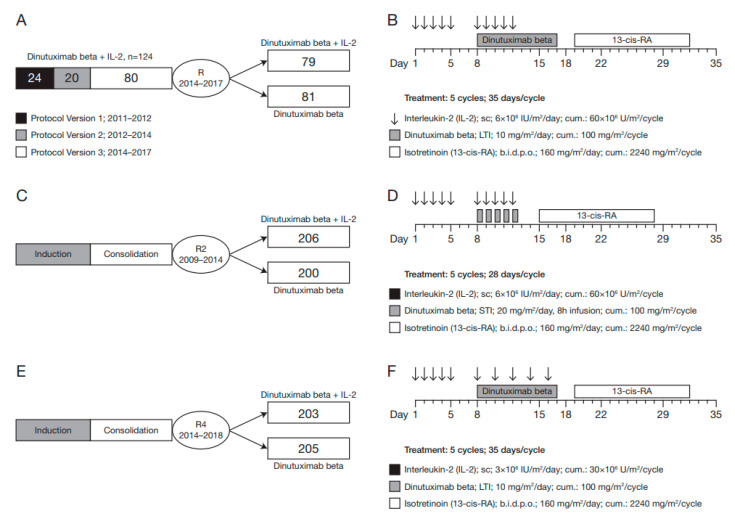
Neurotoxicity is an off-tumour, on-target side effect of GD2-directed immunotherapy with monoclonal antibodies. Here, we report the frequency, management and outcome of patients enrolled in two prospective clinical trials who experienced severe neurotoxicity during immunotherapy with the anti-GD2 antibody dinutuximab beta (DB) administered as short-term infusion (HR-NBL1/SIOPEN study, randomisation R2, EudraCT 2006-001489-17) or as long-term infusion (HR-NBL1/SIOPEN study, randomisation R4, EudraCT 2006-001489-17 and LTI/SIOPEN study, EudraCT 2009-018077-31), either alone or with subcutaneous interleukin-2 (scIL-2). The total number of patients included in this analysis was 1102. Overall, 44/1102 patients (4.0%) experienced Grade 3/4 neurotoxicities (HR-NBL1 R2, 21/406; HR-NBL1 R4, 8/408; LTI study, 15/288), including 27 patients with severe neurotoxicities (2.5%). Events occurred predominantly in patients receiving combined treatment with DB and scIL-2. Neurotoxicity was treated using dexamethasone, prednisolone, intravenous immunoglobulins and, in two patients, plasmapheresis, which was highly effective. While neurological recovery was observed in 16 of 21 patients with severe neurotoxicities, 5/1102 (0.45%) patients experienced persistent and severe neurological deficits. In conclusion, severe neurotoxicity is most commonly observed in patients receiving DB with scIL-2. Considering the lack of clinical benefit for IL-2 in clinical trials so far, the administration of IL-2 alongside DB is not recommended.
神经毒性是使用单克隆抗体进行GD2定向免疫治疗的一种肿瘤外、靶向性副作用。在此,我们报告了两项前瞻性临床试验中患者的神经毒性发生频率、处理方法及结果,这些患者在使用抗GD2抗体地努图希单抗β(DB)进行免疫治疗期间出现了严重神经毒性,DB的给药方式为短期输注(HR-NBL1/SIOPEN研究,随机分组R2,欧洲临床试验注册号EudraCT 2006-001489-17)或长期输注(HR-NBL1/SIOPEN研究,随机分组R4,欧洲临床试验注册号EudraCT 2006-001489-17以及LTI/SIOPEN研究,欧洲临床试验注册号EudraCT 2009-018077-31),单独使用或与皮下注射白细胞介素-2(scIL-2)联合使用。纳入该分析的患者总数为1102例。总体而言,1102例患者中有44例(4.0%)出现3/4级神经毒性(HR-NBL1 R2组,406例中有21例;HR-NBL1 R4组,408例中有8例;LTI研究组,288例中有15例),其中27例患者出现严重神经毒性(2.5%)。事件主要发生在接受DB与scIL-2联合治疗的患者中。使用地塞米松、泼尼松龙、静脉注射免疫球蛋白治疗神经毒性,在两名患者中还使用了血浆置换,效果显著。21例严重神经毒性患者中有16例神经功能恢复,但1102例患者中有5例(0.45%)出现持续性严重神经功能缺损。总之,严重神经毒性最常出现在接受DB联合scIL-2治疗的患者中。鉴于迄今为止临床试验中IL-2缺乏临床获益,不建议在使用DB的同时给予IL-2。