Marasco Giovanni, Dajti Elton, Serenari Matteo, Alemanni Luigina Vanessa, Ravaioli Federico, Ravaioli Matteo, Vestito Amanda, Vara Giulio, Festi Davide, Golfieri Rita, Cescon Matteo, Renzulli Matteo, Colecchia Antonio
Internal Medicine and Digestive Pathophysiology Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, 40138 Bologna, Italy.
Department of Medical and Surgical Sciences, University of Bologna, 40138 Bologna, Italy.
Cancers (Basel). 2022 Apr 12;14(8):1935. doi: 10.3390/cancers14081935.
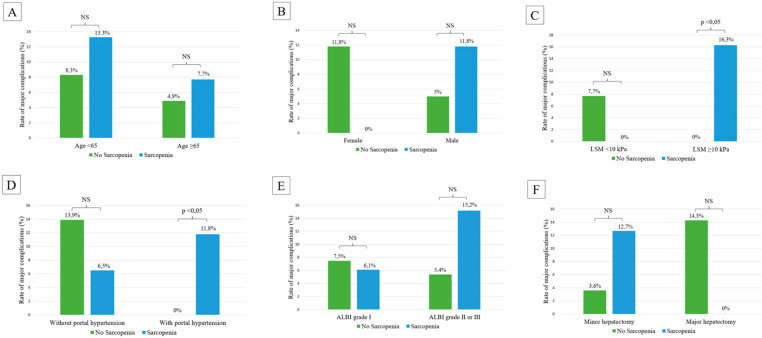
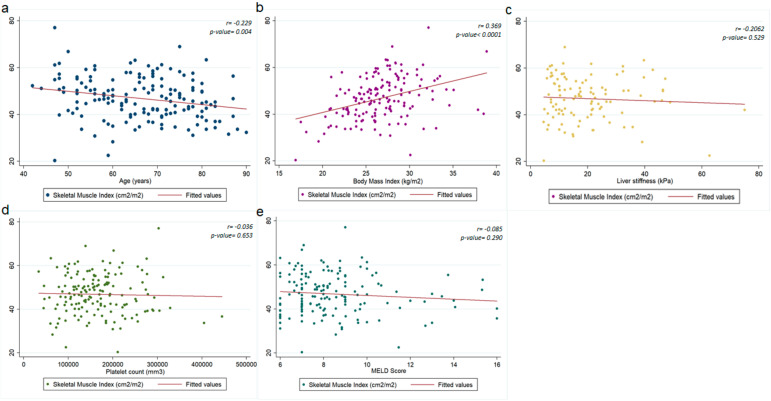
The burden of post-operative complications of patients undergoing liver resection for hepatocellular carcinoma (HCC) is a cause of morbidity and mortality. Recently, sarcopenia has been reported to influence the outcome of patients with cirrhosis. We aimed to assess factors associated with sarcopenia and its prognostic role in liver surgery candidates. We included all patients with compensated advanced chronic liver disease (cACLD) undergoing liver resection for primary HCC consecutively referred to the University of Bologna from 2014 to 2019 with an available preoperative abdominal CT-scan performed within the previous three months. A total of 159 patients were included. The median age was 68 years, and 80.5% of the patients were male. Sarcopenia was present in 82 patients (51.6%). Age and body mass index (BMI) were associated with the presence of sarcopenia at multivariate analysis. Thirteen (8.2%) patients developed major complications and 14 (8.9%) presented PHLF grade B-C. The model for end-stage liver disease score was associated with the development of major complications, whereas cACLD presence, thrombocytopenia, portal hypertension (PH), Child-Pugh score and Albumin-Bilirubin score were found to be predictors of clinically significative PHLF. The rate of major complications was 11.8% in sarcopenic patients with cACLD compared with no complications (0%) in patients without sarcopenia and cACLD ( = 0.032). The rate of major complications was significantly higher in patients with (16.3%) vs. patients without (0%) sarcopenia ( = 0.012) in patients with PH. In conclusion, sarcopenia, which is associated with age and BMI, may improve the risk stratification of post-hepatectomy major complications in patients with cACLD and PH.
肝细胞癌(HCC)患者肝切除术后并发症的负担是发病和死亡的一个原因。最近,有报道称肌肉减少症会影响肝硬化患者的预后。我们旨在评估与肌肉减少症相关的因素及其在肝手术候选患者中的预后作用。我们纳入了2014年至2019年连续转诊至博洛尼亚大学、在过去三个月内进行过术前腹部CT扫描、因原发性HCC接受肝切除的所有代偿期晚期慢性肝病(cACLD)患者。共纳入159例患者。中位年龄为68岁,80.5%的患者为男性。82例患者(51.6%)存在肌肉减少症。多因素分析显示年龄和体重指数(BMI)与肌肉减少症的存在有关。13例(8.2%)患者发生了严重并发症,14例(8.9%)出现了B - C级术后肝功能衰竭(PHLF)。终末期肝病模型评分与严重并发症的发生有关,而cACLD的存在、血小板减少、门静脉高压(PH)、Child - Pugh评分和白蛋白 - 胆红素评分被发现是具有临床意义的PHLF的预测因素。cACLD的肌肉减少症患者严重并发症发生率为11.8%,而无肌肉减少症和cACLD的患者无并发症(0%)(P = 0.032)。在有PH的患者中,有肌肉减少症的患者(16.3%)严重并发症发生率显著高于无肌肉减少症的患者(0%)(P = 0.012)。总之,与年龄和BMI相关的肌肉减少症可能会改善cACLD和PH患者肝切除术后严重并发症的风险分层。